Colleen Huber April 12, 2023 HEALTH VIEWPOINTS,
There are back door routes to the brain. COVID vaccine developers have traversed a path through those doors. And they knew they had entered the brain by November 2020, before the vaccine rollout.
We have 86 billion neurons in the human brain, and each of those connects with 10,000 other neurons. No other structure in the known universe rivals the brain’s complexity.
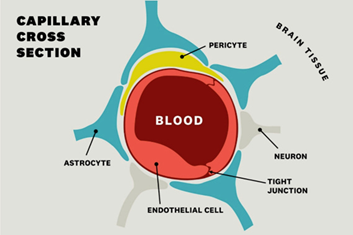
The brain is also the most exclusive club, so to speak, in the body. The gatekeeper is the blood-brain barrier (BBB). That barrier, shown in the second illustration below, is mostly composed of tight junctions between endothelial cells that line, in a single layer, the capillaries (our smallest blood vessels) that nourish the brain. So the BBB is in effect the capillary walls and the tight junctions between its cells.
However, to some extent, there is a liquid component to the BBB, in that the pristine cerebrospinal fluid (CSF) that bathes the brain and spinal cord is kept pure by the BBB. At the risk of oversimplifying, if the central nervous system, which includes the brain and spinal cord, is the royalty of the body, then the skull and vertebrae and BBB are the castle walls, and the CSF is the moat—but a clean moat—unlike the medieval ones. Intruding molecules and pathogens would have to traverse both solid and liquid barriers.
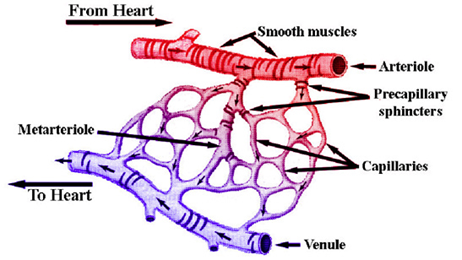
Capillaries are the smallest blood vessels, and they are everywhere in the body. They are the U-turn points where arteries and then smaller arterioles give way to capillaries, then venules, and then veins in blood’s perpetual round-trip from the heart to everywhere else and back again. Anywhere you can point to on your body has a dense and intricate network of capillaries under the skin.
The bottleneck of the BBB is comprised of the tight junctions between capillary wall endothelial cells, prohibiting passage of most substances, as detailed below. Those ubiquitous capillaries run through the entire body, and in the brain they are 40 micrometers apart, which is a space in which two neurons can fit. [1] So every neuron in the brain is nourished by an adjacent capillary.
The Bottleneck at the Blood-Brain Barrier
For a molecule floating in the blood to travel from the blood to a neuron, it has the tightest challenge at the tight junctions between capillary endothelial cells, to exit the bloodstream. Then, once inside the brain, in the space surrounding neurons, if a molecule or a microbe is to arrive into the brain, it must next cross the brain cell (neuronal) membrane to enter that cell, and finally the nuclear membrane of the neuron.
The BBB rejects 98 percent of even small molecules and more than 99 percent of large molecules. [2] Charged or polar molecules and ions cannot pass. The large ones cannot pass directly, simply for not making it past the tight filtration of the BBB. Oils, and substances that are soluble in oils, such as caffeine and nicotine, have a better chance of crossing the blood brain-barrier than water-soluble compounds. Certain small molecules may enter unchaperoned, such as oxygen and glucose. Nutrients such as B vitamins enter by way of saturable transport systems. [3]
Ions and charged polar molecules cannot cross, because they get stuck at the hydrophobic lipid layer. This simply means that because oily and watery fluids do not mix well, the fatty cell membrane disallows passage of most water-soluble substances, and keeps them out of the brain’s cells, unless they are carried in by other means.
But there are back door routes to the brain, and it seems certain that COVID vaccine developers have either arrived there inadvertently or have determined a path through those doors.
And they knew they had entered the brain by November 2020, before the December 2020 vaccine rollout to the public.
So let’s look at what gets into the brain and how that happens.
A typical pharmacology strategy to enter the brain is chaperoning, in which substances that do not typically cross the BBB are compounded together with substances that do cross, which may mimic endogenous molecules. Lipid nanoparticles (LNPs) carry medications into cells but rarely cross the BBB alone. Monoclonal antibodies have shepherded LNPs across the BBB. [4] Enzymes interact with cell membranes and can be used. [5]
Also, if previously non-BBB-crossing LNPs are linked to neurotransmitter-derived synthetic lipids, then they can cross the BBB and carry medications or other chemicals with them, and then those LNPs can enter neurons. [6] The reason for this is that neurotransmitters are typically in the brain—and belong in the brain—and generally pass without gatekeeping.
In other words, when a Trojan horse molecule such as an LNP is dressed up with a neurotransmitter that would typically belong in the brain, it fools the blood-brain barrier into allowing passage inside the brain.
Then COVID Vaccine Injection Occurred
COVID vaccines were advertised to “stay in the arm” following intramuscular injection, although the physiology of circulation, as known for centuries, pre-empts any such localization of a liquid in the body. [7]
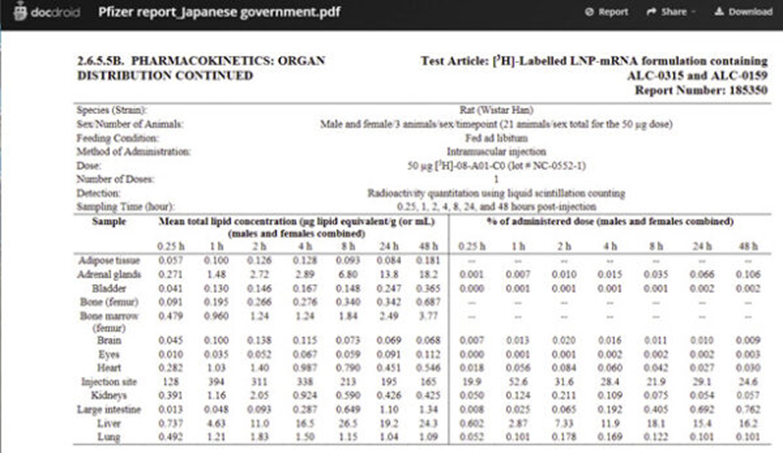
Pfizer contracted with Acuitas Therapeutics in November 2020 to test the Pfizer vaccine in Wistar rats. [8] Their pharmacokinetics report shows that the COVID vaccine LNPs, as well as the messenger RNA (mRNA) they carried, were found within minutes and hours in the brain, eyes, heart, liver, spleen, ovaries, and other organs of the rats, including amounts of mRNA harvested from each sacrificed animal. [9]
Pharmacokinetics studies how much and how fast substances arrive to destinations throughout the body, after intramuscular injection (or other route).
The entire Pfizer report on these findings was submitted by the FDA [U.S. Food and Drug Administration] under court order. [10]
Released by Public Health and Medical Professionals for Transparency. Acuitas Therapeutics. [11] Final Report: Test facility study No. 185350, Sponsor ref No. ALC-NC-0552. Nov 9, 2020. p. 25 https://phmpt.org/wp-content/uploads/2022/03/125742_S1_M4_4223_185350.pdfThis available report text is in Japanese, but the tables at the end are all in English, such as this one. [12]
Other animal studies have shown that when mRNA is packaged in lipid nanoparticles (LNPs), those packets cross the blood-brain barrier. [13] [14] [15] Not only has the mRNA been detected in the brain, but it is also highly inflammatory. [16]
The Pfizer and Moderna COVID vaccines use mRNA to instruct human cells to make spike proteins. Messenger RNA is an intermediary between genes and proteins, in a relationship that is analogous to a template and a finished functional product, where mRNA is the instruction manual. In the case of the mRNA vaccines, spike protein is the product.
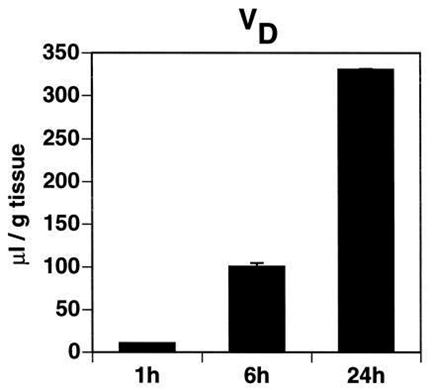
The Pfizer and Moderna vaccines contain pegylated liposome-type LNPs, meaning that they are attached to polyethylene glycol as a chaperone molecule. LNPs are released into the circulation following the vaccine injection, and some of those LNPs approach the blood-brain barrier. It was once thought that LNPs could not cross the BBB unless attached to antibodies, in which case they accumulate in the brain within 24 hours and stay trapped there. [17]
Brain tissue was analyzed at 1 h, 6 h or 24 h after intravenous injection of liposomes packaged with [3H] daunomycin. From J Huwyler, D Wu, et al. Brain drug delivery of small molecules… https://www.ncbi.nlm.nih.gov/pmc/articles/PMC19511/And it is still a challenge for liposomes to cross the BBB. [18] But the mRNA from COVID vaccines have been detected there, as shown above.
Now mRNA Is Inside the Brain and Past the BBB, so It Has Access to Neurons
Now that we have LNPs with their mRNA payload delivered past the BBB and into the brain, what do they do once they arrive to the fluid surrounding neurons? The rest is an easy journey for LNPs. Neurons take up LNPs—and they do so very efficiently, at 100 percent uptake, by means of apolipoprotein E, and usually without immune reaction at that point.
Apolipoprotein E is abundant in the brain—it is produced by astrocytes. [19] [20] The mechanism of uptake is endocytosis, in which the membrane of the neuron engulfs or swallows the approaching LNP. That has been observed since at least 2013. [21] In this way, the Trojan Horse content of the LNP is delivered, because it was contained in a benign-seeming—to the neuronal membrane—package.
A Different Doorway to the Brain
Now at the same time, there is a different process going on. After injection with the mRNA vaccine, LNPs are traveling throughout the whole body, in accordance with long-understood principles of circulation. Cells throughout the body take up these LNPs in endosomes and then the LNPs release their contents (the mRNA payload) into the cytosol of cells, [22] where the mRNA will then instruct the cell’s genetic machinery to produce spike proteins.
Evidence has accumulated that mRNA-generated spike proteins are being produced in various bodily organs following COVID vaccine injection. So throughout the blood, and on toward the brain, there are now free-moving spike proteins on the external side of the blood-brain barrier—that is, in the capillary walls. And it turns out that even they get into the brain. Here’s how the unchaperoned freely moving spike proteins cross the BBB:
Some of those spike proteins are traveling in the circulation and inevitably arrive to the blood-brain barrier. [23] So unlike the LNPs that travel through the membranes of neurons, the spike approaches the blood-brain barrier just as it does in the rest of the body, by way of the ACE-2 receptors, which happen to be abundant at the brain-blood interface. [24] By this route, the S-1 of the spike protein easily crossed the BBB in mice.”[25]
However, the spike protein is toxic in many ways. Each subunit of the spike protein was found to cause a dysfunctional leaking of the BBB. Within 2 hours of spike protein exposure, barrier permeability was seen. [26] It was also found that the spike protein was taken up readily at the capillary endothelial cells of the BBB, which opened that barrier also to spike protein entry to the brain. [27]
So there is an unfortunate feedback loop of earlier-arriving spike proteins widening the gates for later-arriving spikes to enter the brain. The Rho-A molecule seems instrumental in this prying apart mechanism at the tight junctions. [28]
Yet another proposed route of access to the brain is described by Seneff et al., by means of migration of mRNA-containing LNPs via the vagus nerve toward and into the brain. [29]
Brain Injuries Observed by Pfizer
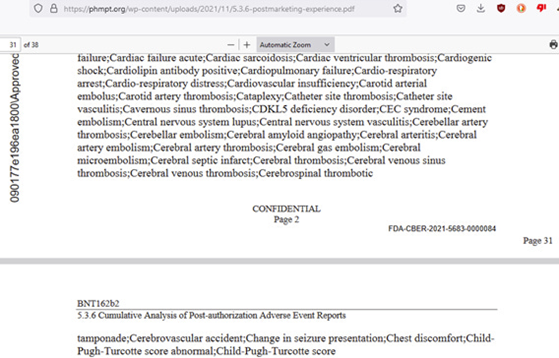
The following screenshot from Pfizer’s documentation to the FDA, released under court order, shows a small part, listed alphabetically, of observed injuries in Pfizer’s clinical trial. [30] Because central nervous system, cerebral, and cerebellar all begin with ce, we can see the injuries they found at the blood vessels of the brain and central nervous system in this one screenshot.

These were injuries found by Pfizer in their 44-thousand-person clinical trial in late 2020. Many of these injuries observed by Pfizer, and submitted to the FDA, in their clinical trial are life-threatening.
For example, cerebral venous sinus thrombosis, which is among those adverse events listed in the screenshot above, is an otherwise rare blood-clotting event that blocks an essential route for blood to exit the brain. As the pressure of blood builds up in the brain, swelling, hemorrhage, and consequent damage to neural structures occur.
You may note that these thrombosis injuries are technically outside the BBB because they occur in a blood vessel. However, any clot in a blood vessel anywhere in the brain has the effect of what is called a watershed infarct. This is what happens in a stroke, or in a smaller injury, a transient ischemic attack.
What this means is that the blood vessel that is blocked by a clot has smaller blood vessels emanating from it in a wedge or pie shape. Now, since the clot became stuck there, all of the tissues in that pie-wedge—the watershed—have been deprived of the oxygen and the nutrients that moving blood would normally bring through those now occluded vessels.
As a result, some tissue inside the blood brain-barrier becomes so damaged that any of the following—memory, cognition, speech, vision, other senses, mobility, and other voluntary muscle control and/or other abilities—can be and are injured—as I will show below.
However, injuries of brain tissue that is protected by the blood-brain barrier are also evident following COVID vaccination, even without detected thrombosis.
Mechanisms of Brain Injury
Peter McCullough, M.D., is the final author on the Seneff, et al. paper, “A Potential Role of the Spike Protein in Neurodegenerative Diseases: A narrative review.” [31]
“Seneff and colleagues describe the pathophysiological rationale for COVID-19 vaccines in the development of neurocognitive disorders. Key features are: 1) CNS penetration of the vaccines, 2) neuroinflammation, 3) Spike protein activation of toll-like receptor-4, 4) folding of Spike protein into amyloid plaques, 5) cumulative exposure with multiple shots connotes enhanced risk.”
“There is now abundant evidence that the synthetic lipid nanoparticles travel into the brain and install the genetic code (mRNA or adenoviral DNA) for the SARS-CoV-2 Spike protein. As this protein is produced and accumulates in the brain, it can cause inflammation and also fold into an amyloid plaque. Thus, there is strong rationale for some vaccine recipients to develop mild cognitive dysfunction, Alzheimer’s like dementia, and other forms of neurocognitive decline. Because seniors were heavily vaccinated, many families and doctors will attribute clinical changes to advanced age and not the vaccine. They should understand in each and every case, that COVID-19 vaccination should be considered a determinant of cognitive decline in a previously healthy person.”
One mechanism of injury to the brain, and all other organs, may be damage to mitochondria observed following COVID vaccination. Abramczyk, et al. showed a reduction in vitro of cytochrome C in mitochondria when exposed to mRNA COVID vaccine. [32] Cytochrome C is essential to oxidative phosphorylation, which is an essential function of mitochondria.
As a result, less ATP [adenosine triphosphate] is produced. ATP is a molecule that is the currency unit of energy in the body. It is used by all cells for energy. When there is less of it, we are exhausted and more vulnerable to cancer among other disease states.
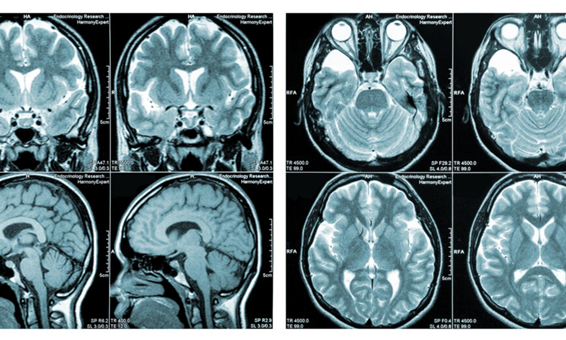
A better known, more easily imaged by MRI, mechanism of injury to neurons is de-myelination. Myelin is the fatty sheath surrounding the axon of each neuron. It enables communication among neurons, with electrical signals leaping quickly along an intact myelin sheath, as when the brain tells the hand to pick up an object, but would get slowed down along damaged myelin.
Breakdown of Types of Neurological Injuries Following the COVID Vaccines
Hosseini and Askari break down four categories of neurological complications of COVID-19 vaccination in the following figure: [33]
Let’s look at the anatomy of a neuron, where we see the long myelin sheath coating the axon, which is the conduit of signaling from one neuron to the next, and on to muscle, which enables activity, or in the opposite direction from skin and sensory organs, eyes, ears, etc., which registers as perceived sensation in the brain.
Myelin is vulnerable to degradation and pitting from a variety of causes, and has been observed following COVID vaccination, [34] as well as earlier vaccines, the effects of which can be seen on MRI. [35] A common manifestation of demyelination is multiple sclerosis (MS). Exacerbation of existing or not yet diagnosed multiple sclerosis was seen after COVID vaccination, [36] as well as new onset MS. [37] [38]
Also observed following COVID vaccination are such demyelinating conditions as Guillain-Barré Syndrome, [39] [40] [41] transverse myelitis, [42] and similar neuropathies. [43]
Guillain Barré Syndrome (GBS) is an auto-immune condition in which the immune system attacks the nervous system—both motor and sensory neurons—causing weakness which may lead to paralysis, as well as tingling and other altered sensations. GBS has long been observed to follow earlier vaccinations, such as Hepatitis B and influenza vaccines, likely due to the upheaval provoked in the immune system by a needle carrying antigenic material past the immune system’s primary defenses in the skin and mucous membranes. Of 1,000 post-vaccine GBS cases reported in the United States from 1990 to 2005, 774 occurred within 6 weeks following vaccination. [44]
© Propel
A Lancet study found that Bell’s palsy has been seen 3.5 to 7 times higher in the COVID-vaccinated population compared to unvaccinated cohort. [45] Bell’s palsy is a dysfunction of the 7th cranial nerve, also known as the facial nerve, and results in facial muscle weakness or paralysis on one side of the face, observed as a one-sided smile or a wink instead of a blink. Abducens nerve (6th cranial nerve) palsy has also been seen following mRNA vaccination. [46] This limits eye movement to the side, affecting peripheral vision.
Encephalopathies [47] and encephalitis [48] and seizures [49] and exacerbation of seizures in epileptics [50] have also been reported following mRNA COVID vaccination.
Functional damage has also been observed following COVID vaccination, even acknowledged in conventional medicine as early as 2021—the year of peak COVID vaccination. [51] [52] Memory loss, aphasia, motor and sensory nerve deficits, muscle weakness, and tremors have been observed following COVID vaccination. [53] [54] [55] [56] [57]
In other cases, worsening of pre-existing neurological pathology has been observed following COVID mRNA vaccination, such as worsening of Parkinson’s Disease [58] [59] and of functional neurological disorder—even in the young. [60]
Of 21 adult patients at a Toronto hospital with functional motor movement disorder, 58 percent developed their neurological symptoms following COVID vaccination, and 22 percent developed such symptoms after COVID infection. [61]
A common complaint reported by clinicians following COVID vaccination is tinnitus, [62] but this is still not well-reported in the medical literature and has circulated anecdotally.
OpenVAERS.com summarizes reports of adverse events following vaccination since 1990 cataloged on the Vaccine Adverse Events Reporting System (VAERS) of the U.S. Department of Health and Human Services. [63] Unlike VAERS, Open VAERS.com summarizes VAERS data by category of injury. [64] For each category of injury and deaths reported to VAERS over its 32-year history, 2021 and to a smaller extent 2022 showed vastly higher number of reports than previously, as the reader can see in the second table below from OpenVAERS that show reports of neurological injuries.
Of the 2.4 million adverse events ever reported to VAERS in its 32-year history, 1.5 million of those events were reported following the COVID vaccines, over their short two-year history.
The following graph shows reports of Guillain Barré and transverse myelitis by year. We can see that 2021, the year of peak COVID vaccine uptake shows far higher incidence than other years.
It is important that copies of studies on the brain injuries and neurological sequelae following COVID vaccines are kept. At a time of rampant censorship in medical publications, many of the studies cited by authors cited here have already been removed from publication and are no longer accessible to the public. Others are behind paywalls, such as this Alonso-Canovas review [65] and many others.
This disappearance of documented vaccine adverse events comes, unfortunately, at a crucial time, as the world begins to consider the magnitude of the effects wrought by the COVID vaccines. Better risk-benefit analyses should be made before future vaccines are rushed into widespread use.