- Karen Bonuck, Qi Gao, Seth Congdon & Ryung S. Kim, Communications Medicine volume 6, Article number: 177 (2026)
Abstract
Background
Five years since the scientific and patient communities first identified the syndrome now known as Long COVID, affected individuals lack treatments, and the US lacks population-based data on its disability burden and correlation with National Institutes of Health (NIH) funding. Moreover, akin to other debilitating conditions it often co-occurs with, e.g., Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and dysautonomia, Long COVID disproportionately impacts females whose concerns are often marginalized.
Methods
We quantify Long COVID years lived with disability (YLDs= prevalence x disability weight) in US adults and its actual/YLD-commensurate average annual NIH FY2022-2024 funding versus 68 comparator conditions, by sex predominance. We derive Long COVID prevalence from Census Bureau surveys (9/2022-8/2023) and apply disability weights from the Global Burden of Disease Study.
Results
Long COVID YLDs approximate those of Alzheimer’s and Asthma. Long COVID received 14% of its disability commensurate funding: $106 million vs. $739.8 million. ME/CFS is the most under-funded condition, receiving <1% of its YLD proportionate funding. Among conditions analyzed, 24 are female-predominant (we estimate Long COVID funding two ways), 12 male-predominant, and 33 show no sex predominance. Among the 12 below-median funded/above-median YLD conditions, 7/12 are female-predominant, none are male-predominant. Median funding/per YLD is 5.2 times higher for male- vs. female-predominant conditions (7.0 vs 1.3 million per YLD, p = 0.007). Overall, YLDs explain 6.5% of funding variance in a linear regression model using YLD as the sole predictor (Adjusted R-squared: 0.065).
Conclusions
With chronic conditions like Long COVID rising, disability burden merits greater consideration in funding decisions, as does biological sex.
Plain language summary
Disability accounts for most Long COVID disease burden, with women most affected. Yet the US lacks data on Long COVID’s disability burden and relative research funding, compared with other conditions. We derived “years lived with disability” (YLDs) for Long COVID in US adults versus other conditions. Long COVID’s disability burden rivals that of Alzheimer’s and asthma. Yet Long COVID receives only 14% of its YLD-proportionate funding—$106 million instead of $739.8 million from the National Institutes of Health (NIH). Conditions affecting mostly men receive 5.2 times more funding/YLD than those affecting mostly women. Overall, YLDs explained just 6.5% of NIH funding levels. Long COVID highlights opportunities for NIH research funding to better align with disability burden and address sex-based disparities.
Similar content being viewed by others

A nationwide study of risk factors for long COVID and its economic and mental health consequences in the United States
Article Open access08 April 2025
Identification of risk factors of Long COVID and predictive modeling in the RECOVER EHR cohorts
Article Open access11 July 2024
Complex patterns of multimorbidity associated with severe COVID-19 and long COVID
Article Open access08 July 2024
Introduction
Long COVID (LC) is a mass disabling event of significant public health concern1,2. Its 200+ associated conditions1,3,4 commonly cluster into fatigue, respiratory and/or cognitive phenotypes5. Known to persist for at least two6,7,8,9,10 to 3 years11 post-infection, The National Academies of Sciences, Engineering, and Medicine defines it is an infection-associated chronic condition following SARS-CoV-2 infection that persists for > = 3 months as “…a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”12 Long COVID is among the chronic, non-communicable conditions that comprise a rising share of disease burden globally13 and in the US14,15. In August 2024– nearly five years after COVID began– 5.3% of US adults were experiencing Long COVID16; 1-in-4 of them consistently report significant activity limitations from its symptoms17. There are still no validated diagnostic markers and treatment protocols for it18. Standard testing routinely yields unremarkable findings despite clear physiological dysfunction1,19. As a result, patient concerns are often dismissed as psychosomatic20, leading to fruitless diagnostic and treatment odysseys1,2,21,22.
The pace, scope and focus of NIH-funded clinical trials for Long COVID has been subject to patient advocates’ and researchers’ critiques2,23. In 2020, Congress announced $1.15 billion for the NIH Researching Covid to Enhance Recovery (RECOVER) initiative; most went towards observational cohort and pathobiology studies (66%), data /management /biorepository costs (19%), and clinical trials (15%).(See: https://recovercovid.org/funding). During a Senate hearing in January 2024, advocates reported being unable to work, attend school or socialize; researchers testified that people with Long COVID “needed treatments yesterday.”2 As of July 31, 2025, just 13/274 (4.7%) of Long COVID intervention studies in ClinicalTrials.gov were NIH-funded [filters applied: seeking + no longer seeking participants; both sexes; all ages; no date limit]. Foreign entities, university and industry sponsored the remaining trials.
The NIH balances multiple factors in setting research priorities and funding decisions: health care costs, scientific opportunity, disease-specific advocacy, novel pathogens and, of course, burden of disease. Disability-adjusted life years (DALYS) are the most common disease burden metric. DALYs combine cause-specific morbidity quantified as “years lived with disability” (YLDs) and mortality measured in “years of life lost” (YLLs). Over the past 20 years, DALYs have accounted for a modest ≈30% (R2) of overall variance in NIH funding24,25,26,27. A 2011 study concluded that “Overall funding levels today are less well aligned with DALYs compared to 10 years ago, suggesting that the IOM’s [Institute of Medicine] 1998 priority-setting recommendations have not been implemented.”25 A subsequent 2008–2019 analysis found that neither DALYs nor changes in DALYs were associated with NIH funding once prior funding levels were included in its models27. This is the first YLD-based disease burden analysis of research funding in the US.
The clinical characteristics of Long COVID overlap with those of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and dysautonomia (particularly its postural orthostatic tachycardia syndrome [POTS] sub-type)1,3,18,28,29,30,31,32,33,34. The risk of both these conditions increases by up to 60% and 80%, respectively, after COVID infection1. All three have shared etiology along with multidimensional, episodic and disabling symptoms; lack treatment protocols; and uncertain prognoses1,3,4,29. Further, all are female-predominant, generate psychological distress, and are often dismissed as psychosomatic1,3,4,29,33. The NIH funds ME/CFS at just 7.3% of its DALYs-commensurate burden35. No such analysis exists for dysautonomia. In about 75% of cases where a disease primarily affects one sex, NIH funding favors males, i.e., female-predominant conditions are under-funded relative to their DALYS, while male-predominant conditions are over-funded35. Notably, our analysis incorporates the first representative prevalence data for the US.
Long COVID often manifests as a debilitating and chronic condition, meeting the definition of chronicity by persisting beyond a year, and necessitating ongoing care and/or limiting daily activities; testimonials confirm this experience2,22,29,32. As a relatively new and complex condition, Long COVID merits scientific commensurate with its burden. To do so, accurately identifying it’s disability burden is “…instrumental to inform health care policy and public health resource allocation.”4 Thus, we quantified Long COVID’s burden of disease for US adults who attribute significant limitations in daily activity to it, i.e., “years lived with disability“ (YLDs= prevalence x disability weight). Prevalence was obtained from Census Bureau’s online Household Pulse Surveys (HPS) from 9/2022 to 8/202336. For Long COVD’s disability weight (0.21) we applied the Institute for Health Metrics and Evaluation/Global Burden of Disease (IHME/GBD) study’s estimate29,37. Next, we compared the YLDs for Long COVID with the NIH’s FY2022-FY2024 funding estimates (average /year) for Long COVID and non-Long COVID comparator conditions and their actual/YLD-commensurate NIH funding, by sex-predominance.
The scientific community first acknowledged the existence of Long COVID in late 202021,38. Here we report the first data on Long COVID disability burden from a representative sample of US adults, and its correlation with annual average NIH funding from 2022-2024 relative to other conditions and biological sex. The disability burden of Long COVID lies between that of Alzheimer’s and asthma. Long COVID received just 14% of its disability commensurate funding: $106 million vs. $739.8 million. Based on a conservative overestimate that includes monies not reflected in the NIH’s funding categories, Long COVID received 53% of its YLD commensurate amount. Similarly, ME/CFS, another female-predominant condition common in Long COVID1 received <1%% of its YLD proportionate funding. Disability burden explained just 6.5% of funding variance overall. However, in gender-specific models only male-predominant conditions showed a small, significant association, explaining 33% of funding variance.
Methods
NIH Funding
We used data from the NIH’s Estimates of Funding for Various Research, Condition and Disease Categories (RCDC) report which provides prevalence, mortality, and DALYs for ≈75 RCDCs. (https://report.nih.gov/funding/categorical-spending#/).We calculated average annual funding as: [(FY 2022 + FY 2023 + FY 2024)/3] based upon the RCDC website as of February 25, 2025 (Supplemental Data 1). We selected these ≈75 RCDC categories as non-Long COVID comparator conditions (except for ME/CFS, see below) because they were the only RCDC conditions that could be mapped to corresponding disease burden measures from the IHME/GBD Study. Throughout FY2022-FY2024, funding was stable across most of the RCDCs, with minimal year-to-year variation observed in all but a few conditions (Supplementary Fig. 1).
For Long COVID (only), we also provide a “holistic” estimate: it includes RECOVER monies not reflected in the RCDC because they were an emergency supplemental appropriation to the Department of Health and Human Services. Absent a public record of exactly when and how much of RECOVER’s $1.15 was allocated and appropriated, we assume $287.5 million/year funding from 2022-2025 (i.e., $1.15 billion/4 years, per communications with US Senate Health, Education, Labor and Pension staff)39. As the only condition for which we include non-RCDC funding data, this “holistic” value represents a conservative overestimate. Given federal funding shifts under the new administration in 202540, we based our RCDC (only) ($106.3 million) and “holistic” analyses ($106.3 million + $287.5 million = $393.8 million) on the average of FY 2022, FY2023 and FY 202440. See Supplemental Data 1 for RCDC funding for Long COVID and comparator conditions (n = 68) analyzed.
Long COVID Disease Burden
We use YLD (“years lived with disability”) to measure the non-fatal disease burden of debilitating Long COVID. We chose YLD over other burden metrics, e.g., DALYs or YLL (years of life lost to disease) because (a) disability— not death— now accounts for most COVID burden41, (b) YLDs may be better measures of disease burden for chronic conditions13, which Long COVID has evolved into for many6,42,43,44, and; (c) there aren’t longitudinal data to estimate YLLs. YLD is calculated as:
YLD = prevalence x disability weight
Long COVID Disability Weight
Disability weights represent health loss from non-fatal diseases, where 0 = full health and 1 = death. The IHME/GBD study produces mortality and disease burden (i.e., YLD, YLL, DALY) data from epidemiologic datasets, population surveys, medical records and the scientific literature (https://www.healthdata.org/research-analysis/gbd). They published disability weights for three common symptom clusters following symptomatic COVID-19 in 2020 and 2021: persistent fatigue, cognitive, and respiratory3, and estimate Long COVID’s disability weight as 0.2129,37. This weight– confirmed by IHME/GBD researchers (Sarah Wulf Hanson email to author, 8/3/2023) (Theo Vos emails to author, 8/3/3023 and 1/8/2024)—is slightly lower than the 0.23 from the latter reference37 as new studies were added to the estimate (Theo Vos email to author, 1/8/2024).
Non-Long COVID Disease Burden
We applied the IHME/GBD’s YLDs for US adults > = 20 years (Supplemental Data 2) to those RCDCs that NIH had harmonized with IHME/GBD categories (Supplemental Data 3). In the rare cases when > = 2 IHME/GBD categories were combined to match an RCDC category, their disease burdens were summed (Bochner D, National Institutes of Health, emails on 7/17/2023 and 12/1/2023). Of the RCDC conditions — including LC and ME/CFS (note below), 6 were excluded from analysis: 5 because harmonizing the IHME/GBD and RCDC categories was difficult and thus we couldn’t extract their YLDs (mental illness, heart disease, Injury (total) Accidents/Adverse Effects, cancer, and sudden infant death syndrome), and 1 because its YLD = 0 (Malaria).
Note- Though ME/CFS is not reflected in IHME/GBD data, its clinical overlap with disabling Long COVID and availability of new US prevalence data [total = 1.3%; women = 1.7%, men = 0.9%]45 enabled us to calculate its YLD, based on a disability weight [0.46] from prior research33,46.
Long COVID Case Data Source
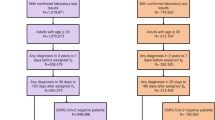
The Census Bureau/Centers for Disease Control and Prevention’s monthly online Household Pulse Survey36 (HPS) from 9/2022-8/2023 was used to identify cases (Supplemental Data 4). This monthly repeated cross-sectional study assesses COVID’s impact from a representative sample of adults (> = 18 years). To harmonize the HPS and IHME/GBD data, we excluded HPS participants < 20 years.
Long COVID Case Definition
The HPS and IHME/GBD both operationalize Long COVID as incident symptoms >= 3 months post- infection but differ in their enumerated symptoms Per above, the LC disability weight of 0.21 is derived from 2020-2021 data for symptoms following symptomatic disease. The HPS symptoms, while less severe than those in the IHME/GBD study, match those enumerated in guidance designating LC as a qualifying disability in the US (https://www.hhs.gov/civil-rights/for-providers/civil-rights-covid19/guidance-long-covid-disability/index.html).
To harmonize differences between the HPS and IHME/GBD symptom descriptions, we restricted our analysis of Long COVID YLDs to just HPS respondents reporting significant activity limitations from Long COVID symptoms. For this case definition respondents had to answer “Yes” to the first three questions below and “Yes, A Lot” to the fourth question:
- 1.Have you ever tested positive for COVID-19 (using a rapid point-of-care test, self-test, or laboratory test) or been told by a doctor or other health care provider that you have or had COVID-19?
- 2.Did you have any symptoms lasting 3 months or longer that you did not have prior to having coronavirus or COVID-19?
- 3.Do you have symptoms now?
- 4.Do these long-term symptoms reduce your ability to carry out day-to-day activities compared with the time before you had COVID-19? (Options: “No, not at all,” Yes, a little” and “Yes, a lot.”)
Sex-Dominant Diseases/Conditions
If a disease or condition affected > = 60% of one biological sex, we classified it as female or male predominant, per prior work35. The remainder were identified as neutral.
Demographics
We describe the aggregate 12-month HPS sample by Long COVID status as a) Current LC Activity Limit: None/A Little, b) Current LC Activity Limit: A Lot (i.e., disabling), c) Past LC and d) Other- never COVID and never LC. Disability status was based on having (any) difficulties seeing, hearing, walking or climbing stairs, remembering or concentrating, doing daily activities and/ or communicating. The HPS incorporated the 2-item Patient Health Questionnaire (for depressive symptoms) and 2-item Generalized Anxiety Disorder scale.
To calculate the prevalence (number of cases per 100,000) of long COVID among adults (age > = 20), 12 monthly data sets collected by HPS spanning 9/2022-8/2023 were pulled together. The replicate weights and base weights were divided by 12; they were then used to calculate the pooled estimate of annual prevalence of Long COVID. The Fay’s modified balanced repeated replication method was used for variance estimation. The YLD of Long COVID was calculated by multiplying the prevalence with the disability weight of 0.21.
Patient descriptive statistics were reported as frequency, weighted frequency and percentage calculated from the pooled data set by using the method for calculating the prevalence of Long COVID. As described above, we calculated the 3-year average (FY2022-2024) NIH funding for Long COVID and non-Long COVID comparator conditions based on RCDC data, as well as a “holistic” estimate for Long COVID inclusive of RECOVER monies.
We show possible associations between the 68 conditions’ 3-year average NIH funding and YLDs in two formats. First, we present the ratio of each condition’s actual/YLD-commensurate average annual NIH FY2022-2024 funding, by its sex-predominance and YLD quartile. Commensurate funding for each condition was estimated by multiplying total average annual funding for the 68 conditions with the proportion of its YLD among the total YLDs. Funding per YLD was calculated by dividing each condition’s actual funding by its YLD. We used a 2-tailed Wilcoxon rank sum test to compare differences in average annual funding per YLD between male vs. female predominant conditions. This comparison includes both the RCDC and “holistic” estimates for Long COVID. Second, we generated a scatter plot with logarithmic scales on both the X (YLD/100,000) and Y axes. Linear regression models were fitted for both male and female dominant conditions by using log transformed 3-year average funding as the outcome, with log transformed YLD as the predictor, and the gender specific regression lines were plotted.
Results
Long COVID Disease Burden v. Other Conditions, by Sex Predominance (Fig. 1)
For context, we present disability weights from the IHME/GBD study for Long COVID and other selected conditions47. Disability weights represent the loss of health from a disease or condition, ranging from 0 (full health) to 1 (death). The comparator conditions were selected to represent a range of disability weights for female-, male- and non-sex-predominant conditions, Long COVID’s disability weight is equivalent to that of traumatic brain injury (0.21), complete hearing loss (0.22) and moderate chronic obstructive pulmonary disease (0.23). It exceeds that of uncomplicated diabetes (0.05) and mild Alzheimer’s (0.07) and is exceeded by symptomatic HIV (0.27), moderate rheumatoid arthritis (0.34) and migraine (0.44). (Fig. 1a). We divided the 69 conditions into YLD quartiles; the highest quartile ranged from 303.7 to 1,444.2. Long COVID had the 16th highest YLD at 320/100,000, just above Alzheimer’s (279.4/100,000) and Alcoholism, Alcohol Use and Health (303.7) and below asthma (355.7) and schizophrenia (397.5). (Fig. 1b)

Characterization of Sample (Table 1)
The sample’s 757,580 US adults completed one of 12 monthly online HPSs between September 2022 and August 2023. Among them, 1.5% (n = 10,401) met our case definition of disabling Long COVID, i.e., reported having Long COVID at the time and experiencing significant limitations to their daily activity attributable to it. Their estimated frequency equates to 3,801,986 U.S. adults. In a prior analysis of HPS data (June 2022–June 2023), prevalence of debilitating Long COVID stabilized after December 202217. And, in HPS data in the 12 months following our analysis (September 2023-August 2024 [the final HPS data collection]) this prevalence averaged 1.5%36, corroborating the stability of our study estimate. Half of respondents with disabling Long COVID were aged 20-49 (n = 4.654, 49.6%). Compared to the overall sample, adults with disabling Long COVID disproportionately identify as female (64.4% vs. 51.4%) and experiencing a disability (80.8% vs. 52.9%), anxiety (57.5% vs.23.8%), depression (51.3% vs. 18.5%) and as having a BA degree (21.1% vs. 32.7%). An additional 4.5% (n = 35,963) had Long COVID with little or no activity limits, yielding an estimated 15 million US adults with Long COVID.Table 1 Sample Characteristics by Long COVID Status, Household Pulse Survey 9/2022-8/2023
Actual/YLD-Commensurate Funding by Conditions’ Sex Predominance and YLD (Fig. 2)
We calculated the ratio of each condition’s actual annual average (FY2022-2024) funding, to what it would receive if NIH funding were allocated proportional to its disability burden. Long COVID was funded at 14% of its 2022–2024 RCDC average actual/YLD-commensurate amount. That is, if Long COVID funding were proportional to its disability burden in US adults, it would have received $739.8 million, versus the RCDC annual average of $106 million. Based on the conservative “holistic’ estimate, Long COVID received 53% of its YLD commensurate amount, i.e., $393.8 million vs. $739.8 million.

Cell shading indicates each condition’s sex predominance i.e., affects > = 60% of one biological sex: red for female (n = 24, including Long COVID “holistic” estimate), blue for male (n = 12), and gray for neither (n = 34). Ordered from lowest to highest actual/YLD-commensurate funding, 6 of the10 lowest funded conditions are female predominant (order; YLD commensurate funding), including ME/CFS (1st; 1%), Gall Bladder disease (7th; 9%), Long COVID (8th; 14%), and Anxiety (10th; 17%). None were male predominant. Among the 10 highest commensurately funded conditions, 6/10 were male predominant, including: HIV/AIDS (61st; 2,600%), Liver Cancer (64th; 2,900%), and Tuberculosis (68th; > 17,000%). None were female predominant.
Actual/YLD-Commensurate Funding by Conditions’ Sex Predominance and YLD: Scatterplot (Fig. 3)
We visualized the Long COVID and comparator conditions by YLDs/100,000 (X axis), and NIH average annual FY2022-2024 funding in millions of US$ (Y axis).The scatterplot is bisected at the vertical median for YLD at 48.4 and at the horizontal median at 244.8 million. Long COVID (RCDC only) appears in the lower right quadrant with the 11 other conditions that were underfunded relative to YLD. Of that quadrant’s 12 conditions, 7/12 are female-dominant, none are male-dominant. Based on the “holistic” estimate, Long COVID falls into the upper right quadrant of conditions with both above median YLD and funding.

Overall, funding and YLD have a small but statistically significant association (Spearman correlation = 0.31, p = 0.009). A linear regression model run to examine the association between actual funding and YLD in log scale, also showed a small but significant association (β = 0.19, p-value = 0.019, R-squared = 0.065). Gender specific linear regression models were run for male- and female-dominant conditions. Only male-dominant conditions showed a significant (albeit small) association between actual funding and YLD (β = 0.27, p-value = 0.029, R-squared = 0.33).
Median Funding Per YLD, by Sex-Predominance of Condition (Fig. 4)
We compared conditions’ sex-predominance by their median (IQR) annual NIH FY 2022-2024 funding. Conditions classified as male- (n = 12) predominant received 5.2-fold more median funding per YLD than those conditions classified as female- (n = 23) predominant: $7.03/YLD [IQR: $3.10–$84.57] vs. $1.29/YLD [IQR: $0.52–$7.05], p = 0.0096). Median funding for the 34 neutral conditions was $6.29/YLD [IQR: $1.00– $27.24]-in-between that of male- and female-predominant conditions.

Discussion
Prior funding, rather than disease burden, is perhaps the most significant predictor of NIH spending27. For Long COVID and related conditions such path dependency portends continued under-funding: NIH annual average FY2022-2024 allocations for Long COVID ($106 million), ME/CFS ($13 million) and POTS ($4 million) fell below the per condition median ($245 million). After a January 2024 Senate hearing on Long COVID, the NIH announced a boost to RECOVER funding2. Though welcomed by advocates and experts, concerns remained about its allocation, adequacy. and sustainability48. Subsequently, Long COVID research grants were cut and the Office for Long COVID Research and Practice closed in Spring 202540. Mirin, whose ME/CFS research informed ours, noted that only through happenstance could a merit-driven proposal review system yield a portfolio reflective of disease burden. He posited that conditions with less mature knowledge bases don’t fare as well with reviewers35. This is why Long COVID advocates have urged scientists to build on knowledge from other post-viral conditions and patients’ lived experiences with them1,2,28.
Application of knowledge about complex post-viral conditions towards understanding Long COVID has been minimal1,3,23,28,29,30,31,32,33, likely because Long COVID shares features of many such “contested illnesses”—including ME/CFS, fibromyalgia, migraine, and Lyme disease. All have medically unexplained symptoms, and predominately affect females who have struggled to get medical professionals to believe their complaints20,34. Our findings align with those of Mirin and colleagues: on average, female-dominant diseases- e.g., migraines and CFS– that are under-funded are more severely so than male-predominant ones33,35,46. An NIH Office of Research on Women’s Health official commenting on Mirin’s [gender] disparities findings stated that they “…demonstrate that the funding of research for women is not aligned with burdens of disease.”49 Since then, the NIH established an Office of Autoimmune Disease Research, acknowledging that 80% of autoimmune diseases affect women. (https://orwh.od.nih.gov/OADR-ORWH#card-1244). This may benefit Long COVID, ME/CFS and dysautonomia, which have autoimmune components, but likely won’t match their respective disability burdens.
Even as Long COVID was compelling millions to confront a new disability identity50, NIH designated people with disabilities as a population with health disparities in 202350,51. Following Long COVID, people with pre-existing disabilities report greater overall disease burden10,52 and unmet healthcare needs53 than persons without prior disability50. The designation was intended to allocate funding to reduce the disparate disease burden of disability, and commit the agency to countering ableism and bias. Indeed, the June 2025 update to the NIH’s RCDC website now includes a “Disability Research” funding category for 2024: https://report.nih.gov/funding/categorical-spending#/). However, after a public comment period in 2023 about replacing the NIH mission statement wording from “…enhance health, lengthen life, and reduce illness and disability” to “…optimize health and prevent or reduce illness for all people,” its wording remains unchanged. Were such a shift in language to occur, this could prompt rethinking how much—and which– disease burden metrics factor into funding decisions. Finally, with the designation, persons with disabilities join groups such as racial/ethnic minorities, lower socioeconomic status individuals, rural populations, and sexual and gender minorities51,54. These groups also experience disparities in Long COVID prevalence and access to care4,26,55,56, and are least likely to be included in Long COVID research18.
Our study’s paramount strength is that it fills a gap cited by clinicians and researchers for quantification of Long COVID’s disability burden4. Our YLD-based analysis “meets the moment” in several ways. Key, is that disability now accounts for most COVID disease burden41. More broadly, with improved survival in nearly all causes of death, non-fatal outcomes become more prevalent13,14, and thus important to quantify. Also, our YLD-based analysis is consistent with the recent NIH designation re: disabilities and health disparities. Another strength is that data from the HPS’s repeated cross-sectional survey of population-based samples increases the robustness of our findings. In addition, we note that the federal guidance on Long COVID’s eligibility to qualify as a disability in the US lists the exact symptoms that we used to define disabling Long COVID. This means our findings are directly applicable to US health care policy and public health planning. For example, our results support Long COVID’s full recognition- vs. “qualifying” as a disability in the US.
Our study has limitations. First, as a novel condition lacking long-term mortality data, Long COVID disease burden can only be assessed by YLDs at this time. Still, myriad factors aside from disability affect research funding, including other disease burden metrics (e.g., DALYs), a condition’s newness and/or its place in the funding pipeline, political and advocacy concerns, transmission potential, system strain, and scientific opportunity. While a broader metric inclusive of such factors would yield more comprehensive funding decisions, disease burden—particularly severity-weighted measures that account for both prevalence and individual patient impact—should remain a primary consideration in research allocation57. Second, harmonizing a disability weight for Long COVID from one source (IHME/GBD) with symptoms from another (HPS) introduces complexities. YLDs are a function of frequency and severity. Thus, we conservatively estimated “frequency” by restricting our case definition to only the most significant activity limitations. Third, as a cross-sectional analysis, results should be interpreted with caution. There is limited data on Long COVD prevalence and disease burden beyond ≈2 years6,7,11. Fourth, as noted earlier, DALYs are the most common burden of disease metric. Thus, we lack context for interpreting our finding that YLDs (alone)—exclusive of YLLs– accounted for 6.5% of funding variance. Fifth, our scatterplot and burden commensurate results might look different with comparator conditions other than the subset we analyzed. Finally, as an experimental survey designed for repeated, rapid deployment, the HPS is subject to coverage bias and a low response rate (3.9–7.0%) across cycles17.
Conclusion
The scientific community first acknowledged Long COVD in late 2020, after the patient community collectively defined it on social media21,38. Nearly four million US adults have Long COVID that significantly limits their daily activity- half are under 50 years of age. Its current health and economic burden in the US is estimated at $2.01 – $30.8 billion when symptoms last 1-3 years This may be an underestimate given dysgenic effects from repeated infection and longer term sequelae15. Five years in, treatments remain elusive. In fact, the Multidisciplinary collaborative guidance on the assessment of treatment of Long COVID (2025) states: “current strategies for managing Long COVID focus primarily on symptom-based supportive care.”18 The most pressing research need remains finding safe and effective treatments through well designed trials with standardized endpoints and outcomes40. “Apart from clinical research, addressing Long COVID’s disability burden will require its full recognition as a disability (not just qualification), alongside public health awareness and provider education. More globally we hope our findings impel similar population-based analyses of Long COVID’s disability burden beyond the US.
Data availability
Source data for Figs. 1–4 in Supplementary Data 1 were drawn from the following: NIH funding data by research, condition, and disease categories (RCDC) was obtained from the NIH RCDC website, accessed on February 25, 2025. As the RCDC website was updated and that dataset is no longer available, we provide a copy of the dataset before the update (Supplemental Data 2). NB- the current NIH RCDC website ends at FY 2024. YLDs for US adults were obtained from IHME/GBD Level 3 estimates for 2019, last accessed November 28, 2025. YLD data by region are available from the IHME/GBD website: https://www.healthdata.org/research-analysis/gbd (Supplemental Data 3). We harmonized NIH RCDC funding category names with conditions by their IHME/GBD derived YLDs using the “Report on NIH Funding vs. Global Burden of Disease” which is available at: https://report.nih.gov/report-nih-funding-vs-global-burden-disease (Supplemental Data 4). The prevalence of Long COVID that significantly limits activity came from the US Centers for Disease Control and Prevention Household Pulse Survey available at: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm. Disability weights for health states were drawn from the IHME/GBD47, specifically Table S13 in the publication’s Supplementary file.
References
- Davis, H. E., McCorkell, L., Vogel, J. M. & Topol, E. J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 21, 133–146 (2023).Article CAS PubMed PubMed Central Google Scholar
- Addressing Long COVID: Advancing Research and Improving Patient Care, U.S. Senate, 2023–2024 sess (US Senate Committee on Health, Education, Labor & Pensions). https://www.help.senate.gov/hearings/addressing-long-covid-advancing-research-and-improvin.
- Blitshteyn, S. et al. Multi-disciplinary collaborative consensus guidance statement on the assessment and treatment of autonomic dysfunction in patients with post-acute sequelae of SARS-CoV-2 infection (PASC). PMR 14, 1270–1291 (2022).Article Google Scholar
- Tabacof, L., Nicolau, E., Rivera, A. & Putrino, D. Post-COVID Conditions and Burden of Disease. Phys. Med. Rehabilitation Clin. North Am. 34, 499–511 (2023).Article Google Scholar
- Wulf Hanson, S. et al. Estimated Global Proportions of Individuals With Persistent Fatigue, Cognitive, and Respiratory Symptom Clusters Following Symptomatic COVID-19 in 2020 and 2021. JAMA 328, 1604–1615 (2022).Article PubMed PubMed Central Google Scholar
- Rahmati, M. et al. A systematic review and meta-analysis of long-term sequelae of COVID-19 2-year after SARS-CoV-2 infection: A call to action for neurological, physical, and psychological sciences. J. Med. Virol. 95, e28852 (2023).Article CAS PubMed Google Scholar
- Fernandez-de-Las-Peñas, C. et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: A systematic review and meta-analysis. J. Infect. 88, 77–88 (2024).Article PubMed Google Scholar
- Bowe, B., Xie, Y. & Al-Aly, Z. Postacute sequelae of COVID-19 at 2 years. Nat. Med. 29, 2347–2357 (2023).Article CAS PubMed PubMed Central Google Scholar
- Hou, Y. et al. Global prevalence of long COVID, its subtypes and risk factors: an updated systematic review and meta-analysis. medRxiv. 2025.01.01.24319384 (2025).
- Fleischer, N. L. et al. Long COVID and New Onset Disability Nearly 2 Years After Initial Infection. Am. J. Prev. Med 68, 1168–1172 (2025).Article PubMed Google Scholar
- Bodey, R. et al. How long is long COVID? Evaluation of long-term health status in individuals discharged from a specialist community long COVID service. J Clin. Med. 13, https://doi.org/10.3390/jcm13195817 (2024).
- National Academies of Sciences E, Medicine. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences. The National Academies Press:186 (2024).
- World Health Organization. World health statistics 2023: monitoring health for the SDGs, sustainable development goals. 2023. 19 May 2023. https://www.who.int/publications/i/item/9789240074323.
- Ansah, J. P. & Chiu, C. T. Projecting the chronic disease burden among the adult population in the United States using a multi-state population model. Front Public Health 10, 1082183 (2022).Article PubMed Google Scholar
- Bartsch, S. M. et al. The Current and Future Burden of Long COVID in the United States. J. Infect. Dis. 231, 1581–1590 (2025).Article PubMed PubMed Central Google Scholar
- National Center for Health Statistics. U.S. Census Bureau, Household Pulse Survey, 2022–2024. Long COVID. Accessed 19 March 2026: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm.
- Ford, N. D. et al. Long COVID and Significant Activity Limitation Among Adults, by Age – United States, June 1-13, 2022, to June 7-19, 2023. Morbidity Mortal. Wkly. Rep. 72, 866–870 (2023).Article Google Scholar
- Cheng, A. L. et al. Multidisciplinary collaborative guidance on the assessment and treatment of patients with Long COVID: A compendium statement. PM R. 17, 684–708 (2025).Article PubMed PubMed Central Google Scholar
- Appelman, B. et al. Muscle abnormalities worsen after post-exertional malaise in long COVID. Nat. Commun. 15, 17 (2024).Article CAS PubMed PubMed Central Google Scholar
- Smyth, N. J. & Blitshteyn, S. Language matters: what not to say to patients with Long COVID, myalgic encephalomyelitis/chronic fatigue syndrome, and other complex chronic disorders. Int. J. Environ. Res. Public Health 22, https://doi.org/10.3390/ijerph22020275 (2025).
- Hereth, B. et al. Long covid and disability: a brave new world. Br. Med. J. 378, e069868 (2022).Article Google Scholar
- U.S. Food and Drug Administration. Virtual Public Meeting on Patient-Focused Drug Development for Long COVID (2023).
- Ladyzhets, B. NIH documents show how $1.6 billion long Covid initiative has failed so far to meet its goals. STAT News. https://www.statnews.com/2024/05/31/long-covid-nih-recover-initiative-falls-short-on-causes-treatments/ (2023).
- Nimgaonkar, A. et al. Exploring static and dynamic relationships between burden of disease and research funding in the United States. Health Res Policy Syst. 20, 60 (2022).Article PubMed PubMed Central Google Scholar
- Gillum, L. A. et al. NIH disease funding levels and burden of disease. PLoS One 6, e16837 (2011).Article CAS PubMed PubMed Central Google Scholar
- Cohen, J. & van der Meulen Rodgers, Y. An intersectional analysis of long COVID prevalence. Int J. Equity Health 22, 261 (2023).Article PubMed PubMed Central Google Scholar
- Ballreich, J. M., Gross, C. P., Powe, N. R. & Anderson, G. F. Allocation of National Institutes of Health Funding by Disease Category in 2008 and 2019. JAMA Netw. Open 4, e2034890 (2021).Article PubMed PubMed Central Google Scholar
- Bonilla, H. et al. Therapeutic trials for long COVID-19: A call to action from the interventions taskforce of the RECOVER initiative. Review. Front. Immunol.14, https://doi.org/10.3389/fimmu.2023.1129459 (2023).
- National Academies of Engineering Sciences and Math. Long COVID: Examining Long-Term Health Effects of COVID-19 and Implications for the Social Security Administration: Proceedings of a Workshop.https://doi.org/10.17226/26619 (2022).
- Knoop, I. et al. Self-reported symptom burden in postural orthostatic tachycardia syndrome (POTS): A narrative review of observational and interventional studies. Autonomic Neurosci. 244, 103052 (2023).Article Google Scholar
- Choutka, J., Jansari, V., Hornig, M. & Iwasaki, A. Unexplained post-acute infection syndromes. Nat. Med 28, 911–923 (2022).Article CAS PubMed Google Scholar
- Astin, R. et al. Long COVID: mechanisms, risk factors and recovery. Exp. Physiol. 108, 12–27 (2023).Article PubMed Google Scholar
- Mirin, A. A., Dimmock, M. E. & Jason, L. A. Updated ME/CFS prevalence estimates reflecting post-COVID increases and associated economic costs and funding implications. Fatigue.: Biomedicine, Health Behav. 10, 83–93 (2022).Google Scholar
- Au, L., Capotescu, C., Eyal, G. & Finestone, G. Long covid and medical gaslighting: Dismissal, delayed diagnosis, and deferred treatment. SSM Qual. Res Health 2, 100167 (2022).Article PubMed PubMed Central Google Scholar
- Mirin, A. A. Gender Disparity in the Funding of Diseases by the U.S. National Institutes of Health. J. Women’s Health (Larchmt.) 30, 956–963 (2021).
- Household Pulse Survey, 2022–2024. Long COVID (2024).
- Hanson, S. W. et al. A global systematic analysis of the occurrence, severity, and recovery pattern of long COVID in 2020 and 2021. medRxiv.https://doi.org/10.1101/2022.05.26.22275532 (2022).
- Callard, F. & Perego, E. How and why patients made Long Covid. Soc Sci Med. 268, 113426 (2021).
- Jindal, N. Senior Health Policy Advisor: Senate Commtitee on Health, Education, Labor & Pensions. 2024–2025.
- Venkatesan, P. US Government cuts funding for long COVID research. Lancet Microbe 6, https://doi.org/10.1016/j.lanmic.2025.101166 (2025).
- Smith, M. P. Estimating total morbidity burden of COVID-19: Relative importance of death and disability. J. Clin. Epidemiol. 142, 54–59 (2022).Article PubMed Google Scholar
- Perlis, R. H. et al. Prevalence and Correlates of Long COVID Symptoms Among US Adults. JAMA Netw. Open 5, e2238804 (2022).Article PubMed PubMed Central Google Scholar
- Ma, Y. et al. Long-term consequences of COVID-19 at 6 months and above: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 19, https://doi.org/10.3390/ijerph19116865 (2022).
- Ma, Y. et al. long-term consequences of asymptomatic SARS-CoV-2 Infection: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 20, https://doi.org/10.3390/ijerph20021613 (2023).
- Vahratian, J., Lin, J. M. S., Bertolli, J. & Unger, E. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome in Adults: United States, 2021–2022. NCHS Data Brief. (2023).
- Mirin, A. A., Dimmock, M. E. & Jason, L. A. Research update: The relation between ME/CFS disease burden and research funding in the USA. WORK: A J. Prev., Assess., Rehabilitation 66, 277–282 (2020).Google Scholar
- Global Burden of Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. In: Supplement 1. Table S13. GBD 2019 sequelae hs, health state lay descriptions, and disability weights, editor. Lancet. 2020/10/19 ed2020. p. 1204–1222.
- Cohrs, R. Long Covid research funding at NIH gets a nearly 50% boost. STAT. https://www.statnews.com/2024/02/15/long-covid-nih-funding-boost/ (2024).
- Smith, K. Women’s health research lacks funding – these charts show how. Nature 617, 28–29 (2023).
- Lund, E. M. & Ayers, K. B. Ever-changing but always constant: “Waves” of disability discrimination during the COVID-19 pandemic in the United States. Disabil. Health J. 15, 101374 (2022).Article PubMed PubMed Central Google Scholar
- Reynolds, J. M. National Institutes of Health Designates Disabled People a Health Disparity Population. JAMA Health Forum 5, e241185–e241185 (2024).Article PubMed Google Scholar
- Hall, J. P., Kurth, N. K., McCorkell, L. & Goddard, K. S. Long COVID Among People With Preexisting Disabilities. Am. J. Public Health 114, 1261–1264 (2024).Article PubMed PubMed Central Google Scholar
- Sullivan, D. L., Goddard, K., Kurth, N. K. & Hall, J. P. I’m in Hell …”: Experiences of Unmet Health Care Needs Among People with Pre-Existing Disability and Long COVID. J. Health Care Poor Underserved 36, 572–589 (2025).Article PubMed PubMed Central Google Scholar
- NIH designates people with disabilities as a population with health disparities. https://www.nih.gov/news-events/news-releases/nih-designates-people-disabilities-population-health-disparities. (2023).
- Tanne, J. H. Covid-19: US studies show racial and ethnic disparities in long covid. Br. Med. J. 380, 535 (2023).Article Google Scholar
- Cohen, J. & Rodgers, Y. V. M. Long COVID Prevalence, Disability, and Accommodations: Analysis Across Demographic Groups. J. Occup. Rehabil. 34, 335–349 (2024).Article PubMed PubMed Central Google Scholar
- Millum, J. Should health research funding be proportional to the burden of disease? Politics, Philos. Econ. 22, 76–99 (2023).