https://doi.org/10.1093/infdis/jiaf030
Background
Long coronavirus disease (COVID), which affects an estimated 44.69–48.04 million people in the United States, is an ongoing public health concern that will persist as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continues to spread.
Methods
We developed a computational simulation model representing the clinical course, health effects, and associated costs of a person with long COVID.
Results
Simulations show that the average total cost of a long COVID case can range from $5084–$11 646 (assuming symptoms only last 1 year) with 92.5%–95.2% of these costs being productivity losses. Therefore, the current number of long COVID cases could cost society at least $2.01–$6.56 billion, employers at least $1.99–$6.49 billion in productivity losses, and third-party payers $21.0–$68.5 million annually (6%–20% probability of developing long COVID). These cases would accrue 35 808–121 259 quality-adjusted life-years (QALYs) lost and 13 484–45 468 disability-adjusted life-years (DALYs) and would rise as COVID-19 incidence increases.
Conclusions
The current health and economic burden of long COVID may already exceed that of a number of other chronic diseases and will continue to grow each year as COVID-19 cases increase. This could be a significant drain on businesses, third-party payers, the healthcare system, and society.
Long COVID has been a growing public health concern as it already affects an estimated 44.69–48.04 million people in the United States (US) [1–3]. Long COVID, as defined by the Centers for Disease Control and Prevention (CDC), is when 1 or more symptoms of acute COVID lasts >3 months even as other symptoms resolve [4]. Other names for long COVID include post-COVID conditions, postacute coronavirus disease 2019 (COVID-19) syndrome, long-haul COVID, postacute COVID-19, postacute sequelae of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, long-term effects of COVID-19, and chronic COVID. Long COVID symptoms include general symptoms (eg, tiredness or fatigue that interferes with daily life, postexertional malaise), respiratory and heart symptoms (eg, difficulty breathing, chest pain), neurological symptoms (eg, brain fog, headache, depression, or anxiety), digestive symptoms (eg, diarrhea, stomach pain), and other symptoms (eg, joint or muscle pain, rash) [4].
Studies have suggested that anywhere from 6%–20% of those infected with SARS-CoV-2 will go on to develop long COVID [5–7]. Since SARS-CoV-2 is expected to continue circulating throughout the US, the number of people suffering from long COVID will continue to grow with each passing year, adding to the already significant total that has resulted from the COVID-19 pandemic. This growing health and economic burden could have major ramifications on employers, insurers, the healthcare system, and to society. To better understand and quantify this burden, we developed a computational simulation model of SARS-CoV-2 infections and the resulting clinical and economic impact of long COVID.
METHODS
Model Structure
We developed a computational simulation model in Microsoft Excel (Microsoft Corporation) with the Crystal Ball add-in (Oracle) that represents the clinical course, the health effects, and the associated costs of a person with long COVID as defined by the CDC [4]. Figure 1 outlines the structure of the model. Each individual (with an age, sex) starts the model as initially infected with SARS-CoV-2. He/she has a probability of developing long COVID (ie, 1 or more symptoms of COVID present >3 months after infection). If he/she develops long COVID, he/she has probabilities of experiencing each of the 19 different long COVID symptoms identified by the CDC [4] (Supplementary Table 1). Thus, this person could develop at least 1 or more specific long COVID symptom, and the person’s chance of experiencing 1 symptom does not affect their chance of experiencing any other symptom.
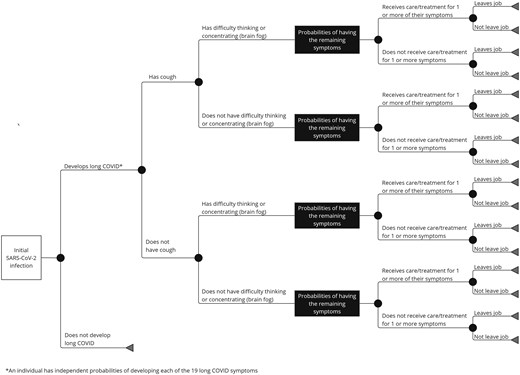
Figure 1.
Model structure. *An individual has independent probabilities of developing each of the 19 long COVID symptoms. Abbreviation: SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
{kind=link}
In the model, each of a person’s symptoms last for a duration drawn from 1 of 3 distribution of lengths derived from previous studies [8, 9] based on early/middle/latter symptoms (Supplementary Table 2) and the longest possible duration of symptoms (which was varied in sensitivity analyses). Each person has a probability of seeking care and being treated for their symptoms. Additionally, each person with long COVID has a probability of missing work/school days and having reduced productivity while at work/school, and those aged 18–64 years old also have a probability of leaving the workforce due to their symptoms for the duration of their symptoms.
Economic Measures
A person accrues different associated direct medical costs (eg, outpatient visits, emergency department visits, inpatient hospital stays, medications, testing) and indirect costs (eg, productivity losses due to absenteeism and presenteeism) based on their long COVID symptoms. Daily wages across all occupations [10] serve as a proxy for productivity losses. Absenteeism results in productivity losses for the duration of days missing work or school. As has been previously done [11–13], we assume that lower utility weights, which estimate functioning compared to perfect health, would correspond to higher presenteeism. This means that a person functioning at 75% compared to perfect health would experience a 25% decrease in productivity while working. For example, presenteeism is correlated with utility weights for anxiety and depression [14]. We attenuated wages by symptom-specific disability weight for the duration of reduced productivity (assumed to be the days with long COVID symptoms minus days absent) as proxy for productivity losses due to presenteeism. Each person has a probability of leaving his/her job due to any of their long COVID symptoms, regardless of whether they seek care for their symptoms. If the person leaves his/her job, they continue to accrue absenteeism productivity losses for the remainder of their symptoms. Since total costs accrue over a year for each symptom and individuals can leave their jobs at any point in the year, rather than track exact dates when they leave, we assumed that the costs would be, on average, half the annual costs across a large population (ie, half cycle correction, to be conservative). We assumed every person accrues productivity losses as all individuals contribute to society.
If a person seeks care/treatment, he/she accrues the average direct medical costs reported in the scientific literature (Supplementary Table 2) for his/her symptom(s). We used the reported costs due to high variability in care and treatment across individual patients. For example, there is not a typical anxiety or depression case as some individuals may use psychotherapy versus medications, and thus, there is no typical treatment. By using a distribution of costs from the literature, we are able to capture this variation in treatment and the spectrum of possibilities.
We measured health effects in both quality-adjusted life-years (QALYs) lost and disability-adjusted life-years (DALYs). Each long COVID case loses QALY values based on age-dependent healthy QALY value and symptom-specific utility weights for the duration of their symptoms. We identified utility weights, using the Tufts Cost-Effectiveness Analysis Registry [15], searching for studies on health conditions that may reflect each long COVID symptom. We conducted a modified Delphi panel with experts selecting the most appropriate studies from which distributions of weights were created. We performed a similar exercise for disability weights using the Global Burden of Disease 2019 study [16]. DALYs are the sum of the years of life lived with disability (YLD) and years of life lost (YLL). However, as we assume that a person could not die directly due to their long COVID symptoms, our DALY calculation did not include YLLs and was therefore:
DALYs = YLD = number of incident cases * disability weight * average duration in years.
If a person had multiple long COVID symptoms, that person accrued the costs for the outcome with the highest direct medical costs and productivity losses, and health effects for the symptoms resulting in the worse health effects. All costs and health effects are presented in 2024 net present value, with past and future values converted using a 3% discount rate.
Once the costs per individual case of long COVID were calculated, each cost (productivity losses, direct medical costs, QALYs lost, DALYs accrued) were then turned into distributions and used as inputs to calculate the current burden of long COVID across the population. Using incidence data from the CDC from 2020–2024 for SARS-CoV-2 [17], we modeled different long COVID scenarios varying the maximum duration of long COVID symptoms, incidence of long COVID [5–7], and adjustments for underreporting of SARS-CoV-2 infections [18–20].
Data Sources
Supplementary Tables 1 and 2 show the key inputs, parameters, values, and sources. When available, all inputs were age- and sex-specific and came from national databases and scientific literature. The historic number of SARS-CoV-2 cases came from the CDC, reported as of 23 February 2024 [17].
Experiments and Sensitivity Analyses
We used the model to determine the cost per long COVID case as well as the potential cost to the US population. Experiments consisted of Monte Carlo simulations of 1000 trials, varying each parameter across its range (Supplementary Table 2). The initial set of scenarios entailed simulating an individual person with long COVID to determine the cost per case by age and sex. The second set of scenarios determined the current burden of long COVID in the US and sent the reported number of SARS-CoV-2 cases in the population that could possibly have/develop long COVID through the model for their remaining duration of long COVID symptoms. The third set of scenarios determined the potential future burden of long COVID and entailed varying the number of SARS-CoV-2 infections in the population. One-way and 2-way sensitivity analyses varied key parameters including the probability of developing long COVID (1%–40%), duration of symptoms (0.5–5 years), the probability of seeking care for symptoms (up to 2 times higher from baseline a median of 12.4% and 15.8% for males and females, respectively), the probability of leaving one’s job (50%–150% values in Supplementary Table 2), utility weights (±10%) and disability weights (±10%), and the cost of symptoms (±50% of values in Supplementary Table 2). Scenarios evaluating the current burden of long COVID also varied the underreporting factor of cases (1–4.2), given differences in potential reporting over the course of the pandemic.
RESULTS
Burden of Long COVID for an Individual Case
Figure 2 shows the cost and health burden of a given long COVID case by age, sex, and long COVID duration. For example, an adult male, when long COVID lasts 1 year, accrues average costs of $9906 (95% uncertainty interval [UI], $2637–$27 386) of which $9432 was productivity losses (24% absenteeism and 76% presenteeism costs), and results in the loss of 0.21 (95% UI, .08–.40) QALYs and 0.08 (95% UI, .02–.16) DALYs. Overall, productivity losses represented the largest proportion, 92.5%–95.2% of the total cost, varying with age and sex. Costs and health effects of long COVID, based on Figure 2 graphs, increase fairly linearly with the duration of symptoms. For example, for a female adult, every 6-month increase in symptom duration increases costs approximately $5038.
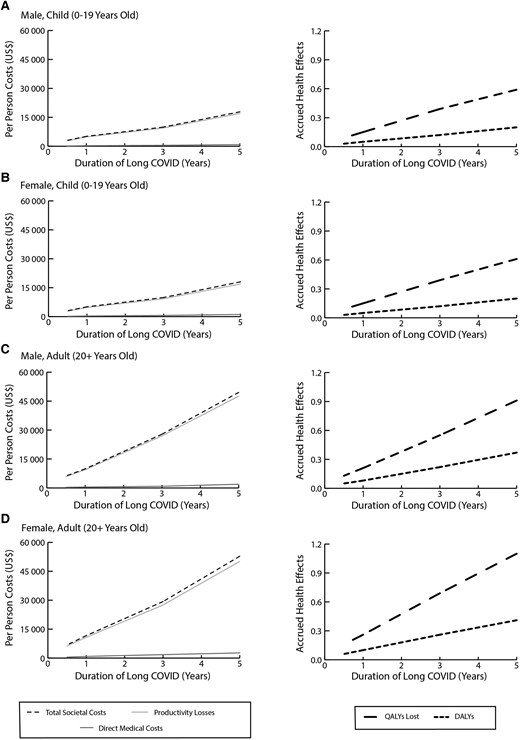
Figure 2.
Costs and health effects per long COVID case and how this varies with the duration of symptoms for a male child (A), female child (B), male adult (C), and female adult (D). Abbreviations: DALYs, disability-adjusted life-years; QALYs, quality-adjusted life-years; US$, United States dollars.
{kind=link}
To represent the fact that some individuals may be more likely to seek care, when we increased the care-seeking probability to twice the currently reported values (eg, to 12.4% for a male, 15.8% for a female), total costs increased by 2.7%–8.2%. For example, for a male child, total costs increased from an average of $5141 to $5282 when their symptoms lasted 1 year. The proportion of total costs due to productivity losses decreased to 87.3%–90.9%.
Since the direct medical costs are from the literature and may include care and treatments specific to other underlying causes of symptoms, we varied these costs to be ±50% of the reported values to help determine the impact of uncertainty in these estimates. While varying these costs impacted the direct medical costs incurred, the impact on total costs is small since productivity losses represent the largest proportion of the burden (eg, 96.4%–97.8% when direct medical costs are 50% lower and 87.5%–92.7% when 150% higher). For example, decreasing direct medical costs by 50% decreased the average total cost per case by 2.5%–6.9% (eg, from $11 646 to $10 848 for a female adult), while increasing them by 150% increases the average cost per case by 0.1%–7.2% (eg, to $12 489 for a female adult).
Given the lack of specific utility and disability weights associated with long COVID and our use of symptom-based proxy studies, we performed additional sensitivity analyses of these parameters. Increasing utility weights by 10% decreased QALYs lost per case by 0.4 for both male and female adults, and by 0.5 per case for male and female children. For example, if the duration of long COVID was 1 year, increasing all disability weights by 10% increased productivity losses for an adult by an average of $921 and $519 per case for males and females, respectively. Increasing disability weights also increased DALYs per case. For example, when long COVID duration was 3 years, increasing disability weights by 10% increased DALYs by an average of 0.2 per case for both male and female adults.
Current Burden of Long COVID
Using the currently reported cases in the US [17] and assuming that the probability of long COVID is 6% and symptoms last 1 year, anyone infected with SARS-CoV-2 since mid-2023 could have or may develop long COVID. Therefore, the current number of long COVID cases (136 739, assuming no underreporting of cases) cost an average of $2.01 (UI, $.93–$3.40) billion and resulted in 35 808 (95% UI, 20 085–53 856) QALYs lost and 13 484 (95% UI, 6935–20 396) DALYs (Figure 3). Direct medical costs comprised 1.04% of the total cost at $20.95 (95% UI, $7.55–$38.26) million and productivity losses comprised 98.96% at $1.99 (95% UI, $.911–$3.38) billion. As Figure 3 shows, the costs and health outcomes increase relatively linearly with increases in the probability of long COVID. For example, when the probability of long COVID is 10%, outcomes are 1.66–1.74 times higher, costing society an average of $3.34 (95% UI, $1.44–$5.53) billion, and resulting in 61 020 (95% UI, 33 053–92 502) QALYs lost and 22 687 (95% UI, 11 987–34 244) DALYs (Figure 3), annually. However, outcomes do not increase linearly with increases in long COVID duration as the number of SARS-CoV-2 cases changed throughout the course of the pandemic and more cases continue to accrue costs for longer and longer symptom durations (Figure 3). For example, when long COVID symptoms last 3 years, anyone infected with SARS-CoV-2 since mid-2021 could already have or may develop long COVID. Thus, with a 6% probability of long COVID, there would be 1 947 419 long COVID cases, costing an average total of $30.8 (95% UI, $14.1–$51.1) billion and accruing 219 135 (95% UI, 122 728–329 534) DALYs for 2024 onward (excluding costs that may have been incurred previously).
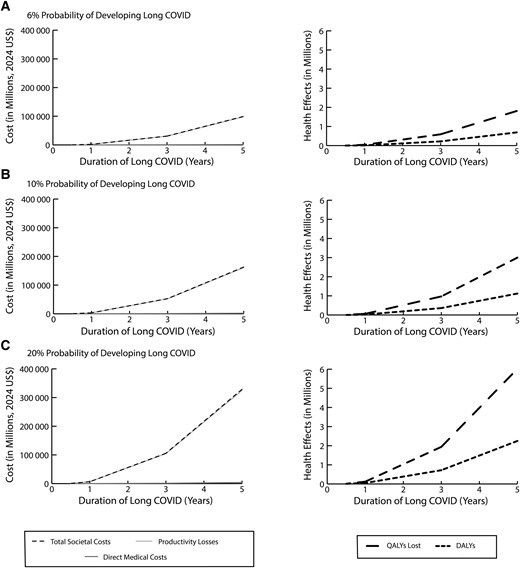
Figure 3.
Current total costs and health effects due to long COVID and how this varies with duration of long COVID when the probability of developing long COVID is 6% (A), 10% (B), or 20% (C). Abbreviations: DALYs, disability-adjusted life-years; QALYs, quality-adjusted life-years; US$, United States dollars.
{kind=link}
Since SARS-CoV-2 cases are underreported, and the level of underreporting varied over the pandemic’s course, we varied the underreporting factor of SARS-CoV-2 infections and found that the burden of long COVID increased proportionally. For example, when SARS-CoV-2 cases are underreported by a factor of 3, there were 410 124 long COVID cases (assuming 6% probability of long COVID, 1 year duration), costing society an average of $5.92 (95% UI, $2.68–$10.01) billion, with productivity losses representing 99% of total costs, and resulting in 109 285 (95% UI, 61 922–165 080) QALYs lost and 41 145 (95% UI, 21 429–62 306) DALYs.
Again, varying the probability of seeking care and direct medical costs did not significantly change the resulting total burden. For example, when individuals were twice as likely to seek care, the average direct medical costs increased to $67.34 million and total societal costs increased to $3.4 million (of which productivity losses represented 98%); thus, total costs increased by 2% (1-year duration, 10% probability of long COVID).
Future Potential Burden of Long COVID
As some individuals recover and others become infected (or reinfected), the number of long COVID cases may vary in the future. Therefore, we quantified the annual burden of long COVID for different SARS-CoV-2 incidence levels in the US population. Figure 4 shows how direct medical costs, productivity losses, total societal costs, QALYs lost, and DALYs accrued varied by incidence of COVID-19 in the US and the probability of developing long COVID (assuming symptoms last 1 year). For example, with an incidence of 100 per 10 000 persons (similar to the incidence reported in 2023; 6% probability of long COVID), annually, long COVID costs society $2.71 billion (95% UI, $1.34–$4.4 billion), resulting in 50 493 (95% UI, 29 116–72 878) QALYs lost and 19 112 (95% UI, 11 030–27 467) DALYs. As Figure 4 shows, costs and health effects increase fairly linearly with increases in incidence. Every 10-point increase in incidence results in an additional $365 million in total annual costs and 5070 additional QALYs lost, and 1900 additional DALYs.
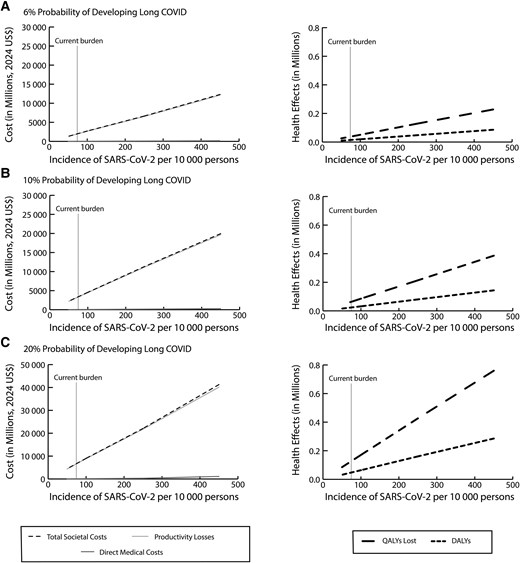
Figure 4.
Impact of varying severe acute respiratory syndrome coronavirus 2 incidence in the population on costs and health effects due to long COVID when the probability of developing long COVID is 6% (A), 10% (B), or 20% (C). Abbreviations: DALYs, disability-adjusted life-years; QALYs, quality-adjusted life-years; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; US$, United States dollars.
{kind=link}
These graphs can be used to estimate the burden over multiple years and for various incidence values over time. For example, if symptoms last 2 years, long COVID would cost an average of $5.42 billion (ie, $2.71 billion × 2) assuming a 100 per 10 000 persons incidence (6% long COVID probability). As another example, with an incidence of 250 per 10 000 persons in year 1 and 100 per 10 000 persons in year 2, long COVID would cost $15.90 billion over the 2-year period, accruing an average of 112 072 DALYs (assuming symptoms last 1 year, 10% probability of developing long COVID).
DISCUSSION
To our knowledge, our study is the first to not only quantify the current health and economic burden of long COVID in the US but also show what the future burden may be and what will drive these estimates. For example, while a cohort study of 138 818 individuals with SARS-CoV-2 infections did show that >80 postacute sequelae of COVID-19 accrue 80.4 DALYs per 1000 people, this study was limited to Veterans Affairs patients who already had long COVID [21]. While claims data analyses have estimated the cost associated with post-COVID-19 infection to be $2683–$12 046 per case [22–24], such analyses have been limited in the populations (eg, only hospitalized patients) and time horizons (eg, 6 months or less) covered and did not include productivity losses, which, as our study has shown, may constitute >90% of the overall costs. Other analyses estimates that long COVID results in $2.6 trillion in expenditures (reduced health, medical care spending, lost earnings) over 5 years [25, 26] focused on particular long COVID symptoms rather than the totality of the condition.
Our results showed that the current economic burden of long COVID could already exceed that of a number of conditions such as carpal tunnel ($2.7–$4.8 billion annually) [27], Lyme disease ($345–$968 million annually) [28], and psoriasis ($35.2 billion annually) [29]. In fact, our study may actually underestimate the burden of long COVID since we endeavored to be conservative with our burden values. For example, we limited our model to the CDC-defined symptoms, while studies have shown that long COVID may be associated with increased risk of heart disease, including myocardial infarction [30] and stroke [31], as well as blood vessel damage in the lungs [32] or brain [33], potentially resulting in gray matter brain degeneration and cognitive decline [34]. Moreover, our study did not account for the potential effects of long COVID on childhood development and education.
The finding that most of the costs come in the form of productivity losses emphasizes how long COVID may already be a significant and growing major employer and workforce issue. The bottom line of companies and organizations as well as the economic stability of the US depend heavily on the health of the workforce. Therefore, it is in the best interest of employers to understand how long COVID may be affecting their employees. However, at the present time, it may be difficult to track and fully appreciate the productivity losses from long COVID since most of these result from presenteeism rather than straight absenteeism. Many employers and other decision makers may not currently have systems in place to properly measure and deal with presenteeism. As indicated earlier, while claims data can offer some insight, they exclusively cover direct medical costs and thus may grossly underestimate the burden of long COVID.
That does not mean that the healthcare systems and third-party payers will not be significantly affected by this growing wave of long COVID cases. Although some healthcare systems have set up special clinics and centers for long COVID, it is not yet clear whether such clinics and centers are enough to deal with all of the long COVID cases and their sequelae and how sustainable these clinics and centers are without additional funding and resources. As can be seen by our study, the health effects of long COVID span different specialties (eg, cardiac, respiratory, neurological) while many specialists have become increasingly siloed. Moreover, it is not clear how many long COVID symptoms will be covered by third-party payers. Many individuals who sought care for long COVID earlier in the pandemic have been left with high medical bills not covered by their insurance or are struggling with care and coverage [35, 36]. Results from our study can help guide reimbursement and coverage policies for long COVID treatment and disability.
Limitations
All models are simplifications of real life and as such cannot account for every possible event or outcome. Cost data were derived from studies of varying quality and rigor; thus, we varied these costs widely in sensitivity analyses to determine their impact on the resulting burden. The definition of long COVID used by this study also may affect the calculated burden; for example, a stricter definition of long COVID would decrease the costs and health effects attributable to long COVID. Additionally, long COVID symptoms may change over time with different SARS-CoV-2 variants. Furthermore, we assumed that the severity of symptoms was steady for the simulated period of time. In reality, these may fluctuate over time, leading to an increase in costs, QALYs lost, and DALYs. Additionally, to be conservative, we did not account for the impact of multiple infections on the probability of getting long COVID, as studies show that subsequent infections increase the likelihood of developing long COVID, which would increase the number of long COVID cases [21, 37].
CONCLUSIONS
Our study has estimated the current burden of long COVID to be on average $2.01–$30.8 billion when long COVID symptoms last between 1 and 3 years. If the future incidence rate and probability of long COVID remain similar to 2023 values (100/10 000 persons and 6%, respectively) for the next 3 years, then total costs may increase to $8.13 billion (UI, $4.02–$13.16 billion). The current health and economic burden of long COVID may already exceed that of other chronic diseases and will continue to grow each year as more and more COVID-19 cases occur. This could be a significant drain on businesses, third-party payers, the healthcare system, and all of society.