
“We know it goes to the brain, it goes to the heart, it produces the spike protein, which damages those cells, causes inflammation… it travels… causing damage to blood vessels and blood clots.”
Authors: Kanekoa Kanekoa News October 6, 2022
Dr. Michael Mörz from the Institute for Pathology in Dresden, Germany, published a case study of an autopsy of a 76-year-old deceased man in the journal Vaccines.
In the report, spike proteins specifically attributed to COVID-19 vaccination targeted blood vessels in the man’s brain and heart.
Incredibly, the report used immunohistochemistry, which uses immune staining methods that light up specific antigens, to determine that “only spike protein but no nucleocapsid protein” could be detected meaning the necrotizing encephalitis (death of brain tissues) as well as the inflammatory changes in the small blood vessels (brain and heart) were caused by COVID-19 vaccination rather than viral infection.
“Surprisingly, only spike protein but no nucleocapsid protein could be detected within the foci of inflammation in both the brain and the heart, particularly in the endothelial cells of small blood vessels. Since no nucleocapsid protein could be detected, the presence of spike protein must be ascribed to vaccination rather than to viral infection. The findings corroborate previous reports of encephalitis and myocarditis caused by gene-based COVID-19 vaccines.”

Interestingly, the elderly man who had Parkinson’s Disease (PD) “experienced pronounced cardiovascular side effects, for which he repeatedly had to consult his doctor” after his first Astra Zeneca ChAdOx1 vector vaccine in May 2021.
After his second vaccination with Pfizer’s BNT162b2 mRNA vaccine in July 2021, the family noticed that the elderly man experienced “increased anxiety, lethargy, and social withdrawal.”
Furthermore, “there was a striking worsening of his PD symptoms, which led to severe motor impairment and a recurrent need for wheelchair support”, which the man “never fully recovered from” before receiving his third vaccination (second Pfizer) in December 2021.
Two weeks after the third vaccination, he “suddenly collapsed while eating dinner” without “coughing or any signs of food aspiration”.
He recovered from this more or less, but one week later, he again suddenly collapsed silently while eating his meal, leading to his hospitalization and death shortly thereafter.
The man’s family asked for an autopsy because he had already shown noticeable changes in behavior, cardiovascular symptoms, and worsening of his Parkinson’s Disease symptoms after each COVID-19 vaccination.
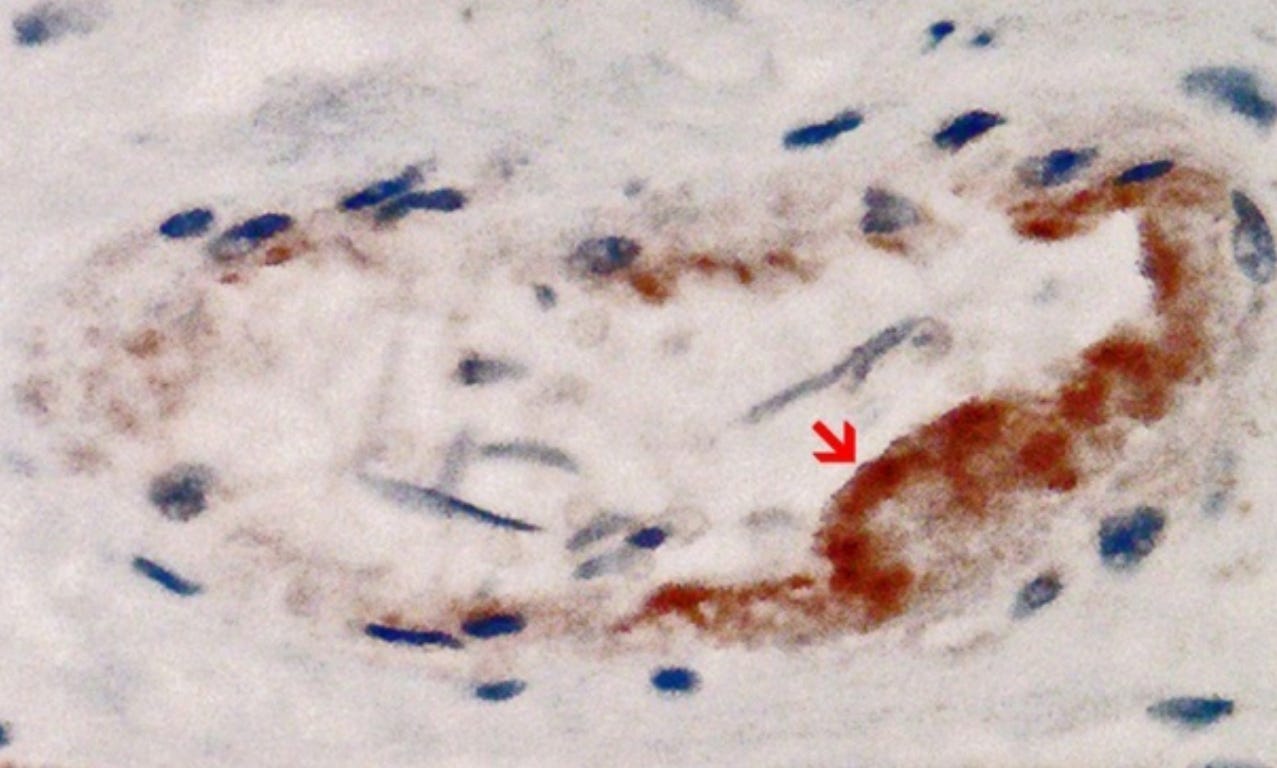
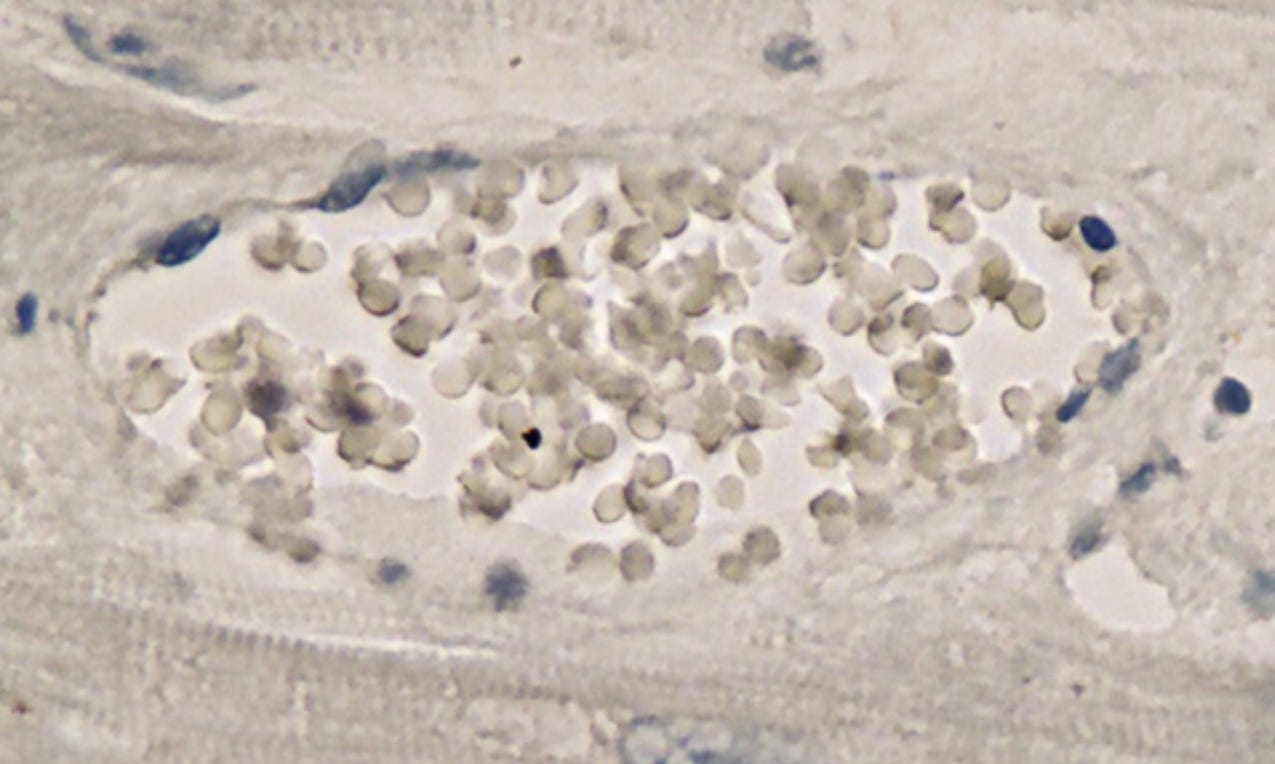
“In the brain, SARS-CoV-2 spike protein subunit 1 was detected in the endothelia, microglia, and astrocytes in the necrotic areas. Furthermore, spike protein could be demonstrated in the areas of lymphocytic periarteritis, present in the thoracic and abdominal aorta and iliac branches, as well as a cerebral basal artery. The SARS-CoV-2 subunit 1 was found in macrophages and in the cells of the vessel wall, in particular the endothelium. In contrast, the nucleocapsid protein of SARS-CoV-2 could not be detected in any of the corresponding tissue sections.”
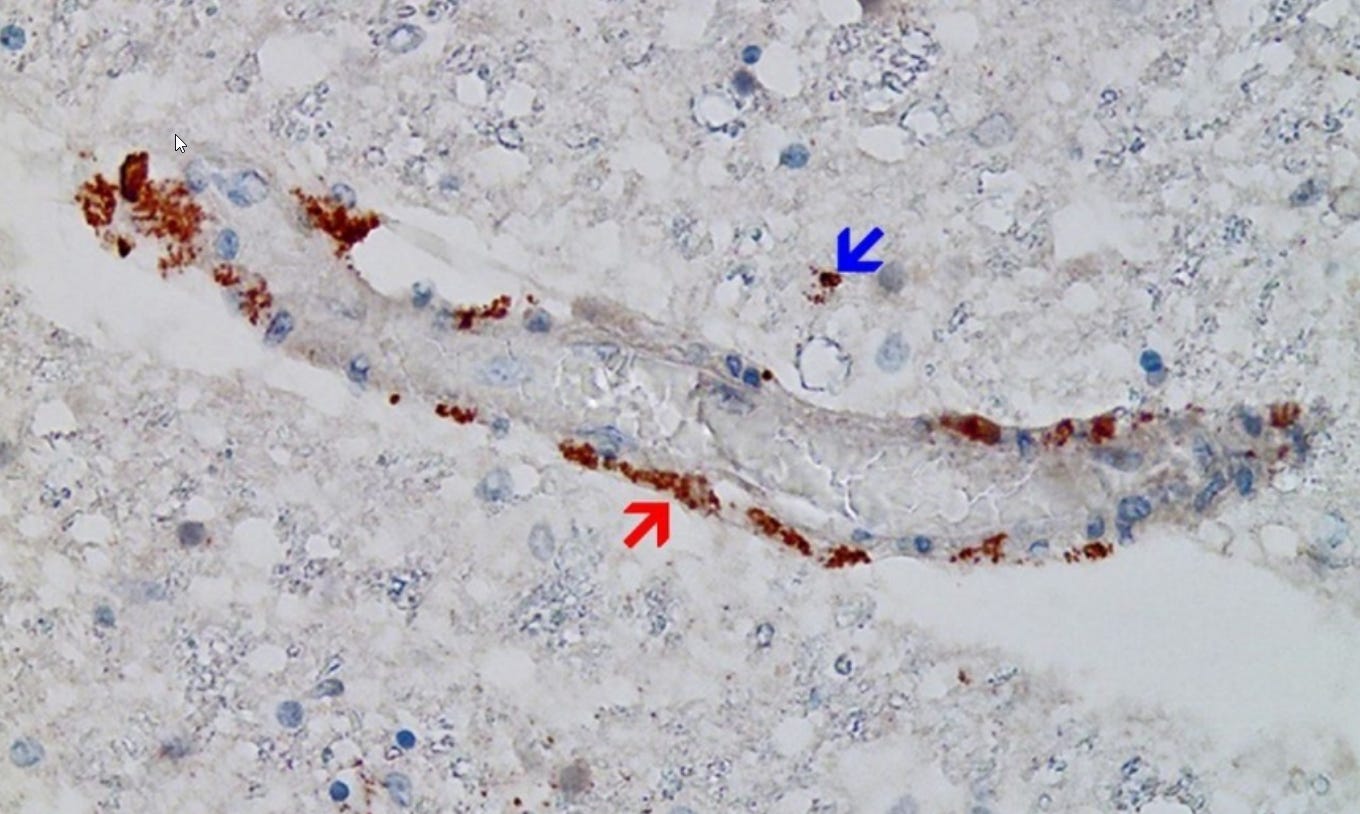
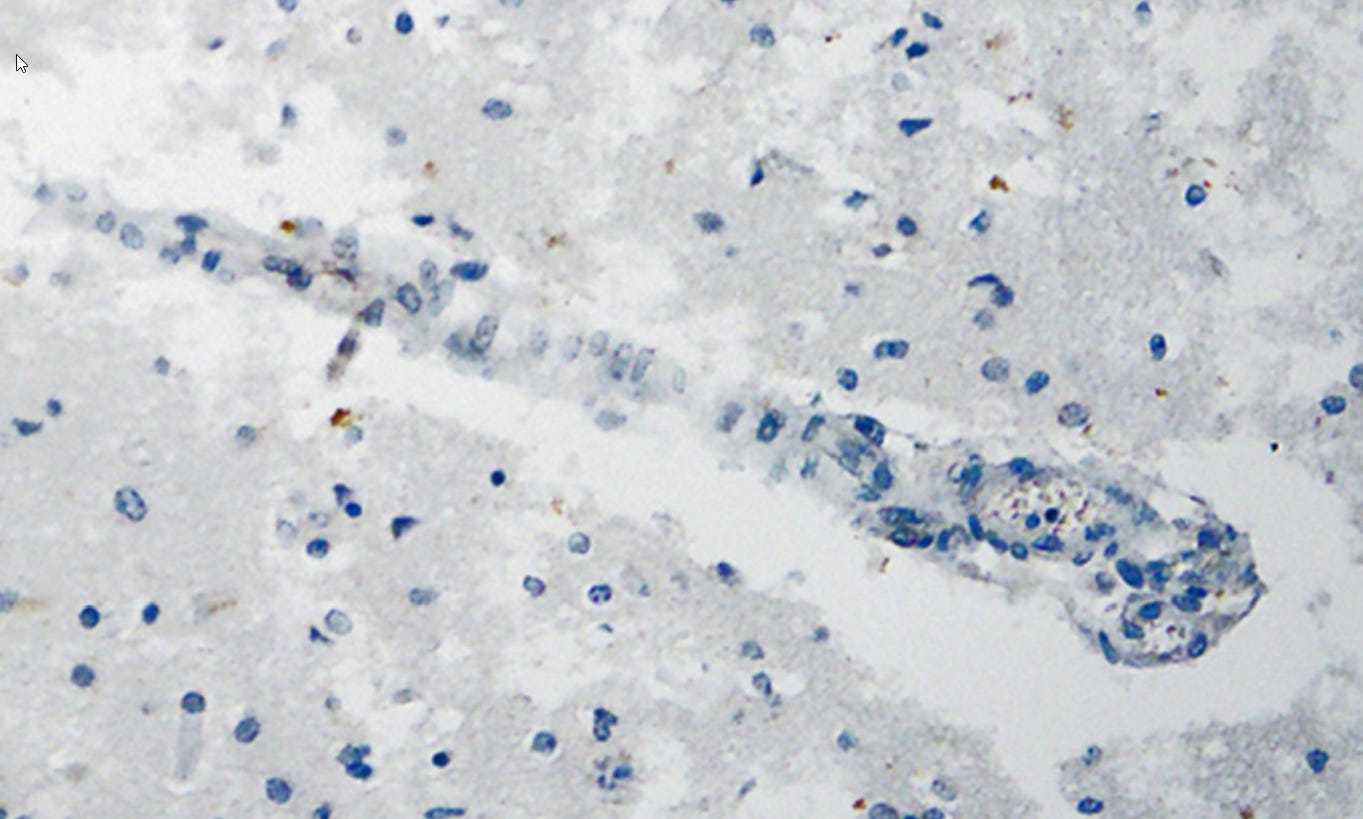
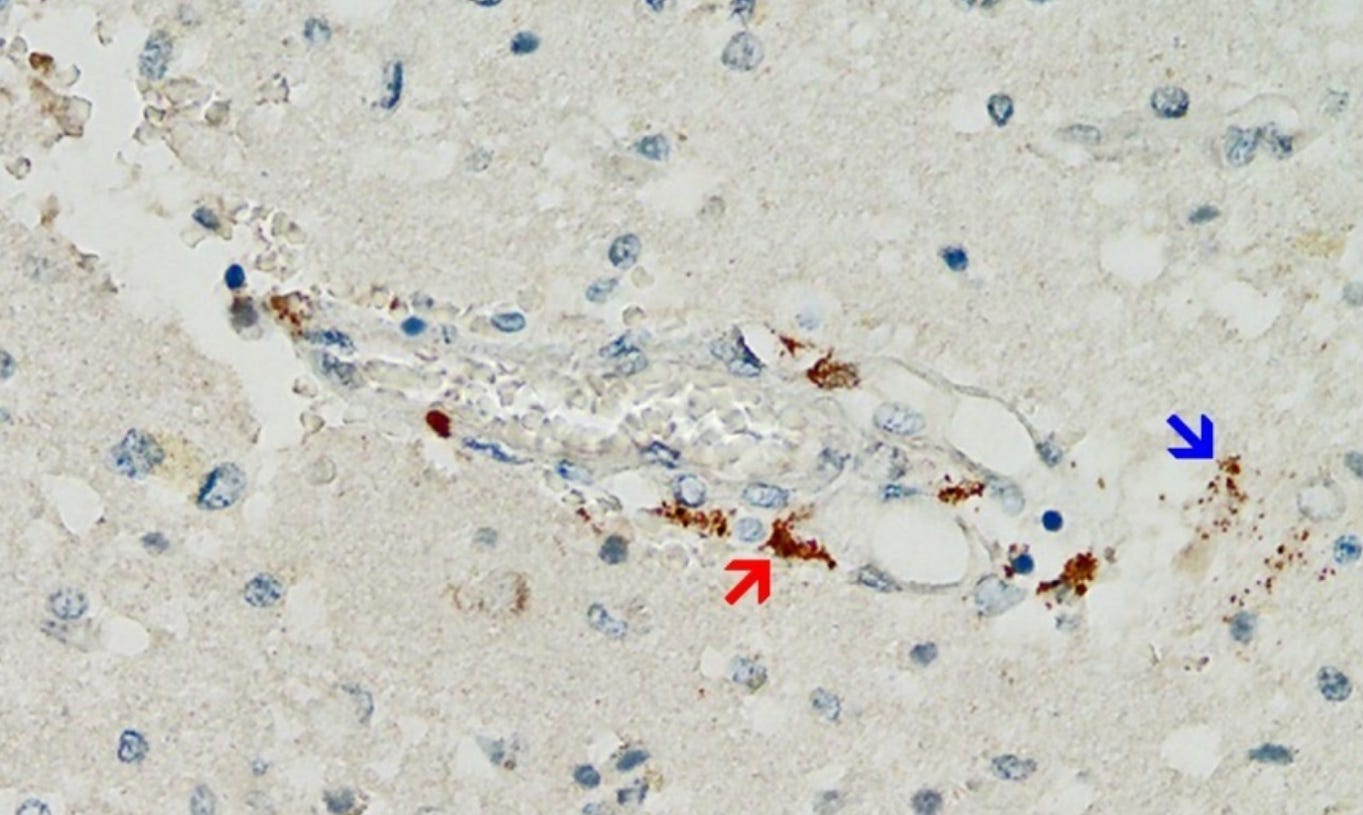

“Immunohistochemistry for SARS-CoV-2 antigens (spike protein and nucleocapsid) revealed that the lesions with necrotizing encephalitis as well as the acute inflammatory changes in the small blood vessels (brain and heart) were associated with abundant deposits of the spike protein SARS-CoV-2 subunit 1. Importantly, spike protein could be only demonstrated in the areas with acute inflammatory reactions (brain, heart, and small blood vessels), in particular in endothelial cells, microglia, and astrocytes. This is strongly suggestive that the spike protein may have played at least a contributing role to the development of the lesions and the course of the disease in this patient.”
Dr. Robert Malone, a critic of the COVID-19 vaccination program, has long warned that the, “synthetic mRNA like genetic material persists in the body for 60 days or longer and produces spike protein at levels higher than is observed with the actual SARS-CoV-2 infection.”
Ominously, the CDC quietly removed the claim that the vaccine generated spike protein “does not last long in the body” from its website between July 16th and July 22nd.
“This is the first time we have had a vaccine go to the brain and go to the heart,” Dr. Peter McCullough, another expert has warned since last year.
“We know it goes to the brain, it goes to the heart, it produces the spike protein, which damages those cells, causes inflammation, and then from there it travels in the body causing damage to blood vessels and causing blood clots.”