Authors: Dr. Yuhong Dong and Health 1+1 via The Epoch Times, October 13, 2022
The Lancet COVID-19 Commission published an article on Sept. 14, 2022 about the lessons learned from the COVID-19 pandemic. As of May 31, 2022, 6.9 million deaths from COVID-19 were reported, but the estimated excess death toll is 17.2 million, based on data from the Institute for Health Metrics and Evaluation (IHME) at the University of Washington. The report states that “this staggering death toll is both a profound tragedy and a massive global failure at multiple levels.”
{kind=link}
The Commission identified six major areas of failures, namely failures of prevention, failures of rationality, failures of transparency, failures to follow normal public health practice, failures of operational cooperation, and failures of international solidarity.
Due to these failures, social sustainability goals were set back a few years and 17.2 million lives were lost.
What can we learn from these failures? I’d like to share my thoughts based on the six failure reasons raised by Lancet.
First Lesson Learned: Failure of Prevention
Many countries adopted aggressive methods to stop the spread of the virus, such as social distancing, lockdowns, vaccines, etc. But none of the methods hit the nail in the head, so to speak.
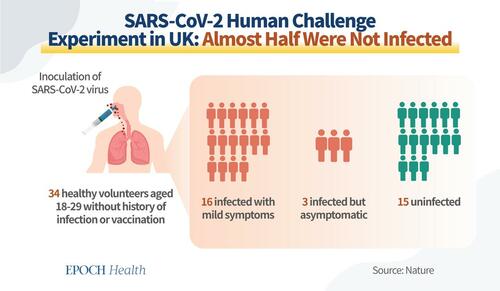
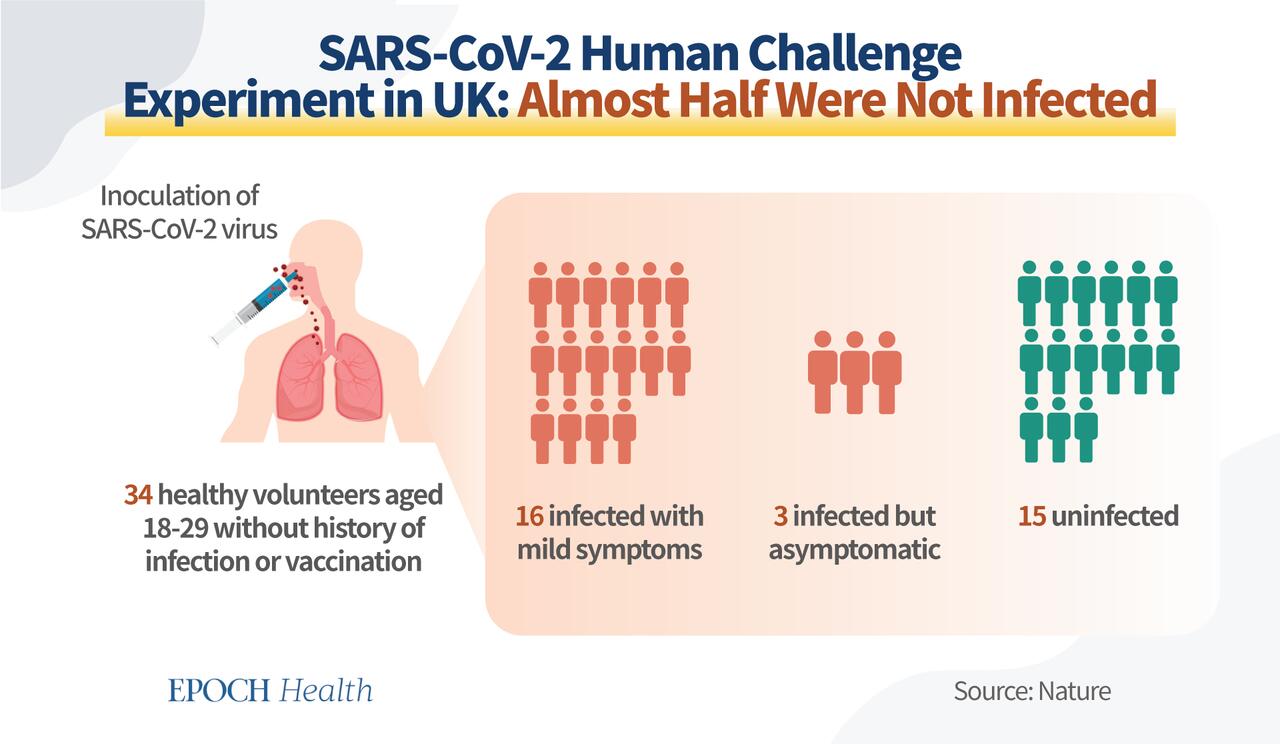
A SARS-CoV-2 human challenge experiment was done among young adults by researchers in the UK. Their paper was published in the March 2022 issue of Nature.
The study involved 36 healthy volunteers aged 18–29 without history of SARS-CoV-2 infection or vaccination. They were inoculated with the SARS-CoV-2 virus intranasally. During the experiment, two were excluded from the Per-Protocol analysis because baseline antibodies were detected. The results of 34 subjects were: 16 participants were infected (confirmed with PCR tests) with mild symptoms, 3 were infected (confirmed with PCR tests) but were asymptomatic, and 15 participants remained uninfected.
{kind=link}
The reason why the 15 participants were not infected should be the key to prevention. In my view, this key is to strengthen people’s immune systems.
Humans have an intricate immune system, a comprehensive defense network against external invading substances. The first line of defense is the physical barriers such as skin, nose hair, tears, etc. They can block most pathogens from entering the body.
The second line of defense is the epithelial interferon barrier. When a virus enters an epithelial cell, the cell automatically activates its antiviral mechanism and produces interferon. Interferon is a natural enemy of viruses and sends instructions to coordinate cells to fight the virus and prevent it from replicating.
Even if the virus enters the blood, there are the innate and adaptive immune cells to protect us. These include the macrophages, dendritic cells, and natural killer cells in the blood, all of which play an important role in antiviral immunity.
No matter what type of disease we are facing, it is important to know that the pathogens are external factors, and it is the human body itself that determines whether we fall ill or not. After we identify and correct the problems in our immune system, those external factors won’t matter much.
Therefore, strengthening our innate immune functions is the key to prevent pandemic spread.
Second Lesson Learned: Failure of Rationality
Rationality refers to the ability to make decisions based on facts. In the process of vaccine development, irrationalities included blindly pushing the vaccine among the masses without a complete evaluation of its efficacy and safety.
There are many limitations with the vaccines.
- Inability to prevent infection: Neutralizing antibodies are mainly produced in the human bloodstream, but not in the epithelial cells. Therefore, if the first two lines of defense were weakened, the virus could still enter the blood and cause infection. That is why the vaccine and antibody strategy is unable to prevent infection.
- Needs to be renewed: Vaccines need to be renewed along with the virus variation, and the current vaccine is designed based on the genetic code of the old strain in 2020.
- Needs time to develop: On average, it takes five to 10 years to develop a vaccine. It requires a significant amount of animal trials and human trials to ensure the vaccine’s safety and prove its efficacy. Viruses mutate quickly. The speed of vaccine development can never match that of the viral mutation. If the vaccine is injected frequently for different variants of the virus, it will generate the antibody-dependent enhancement effect (ADE effect), which makes the vaccine ineffective.
- Inferior to our natural immunity: Numerous studies have shown that the immunity produced by the human body against viruses after natural infection is much longer lasting and stronger than the antibodies produced by simply stimulating T cells with vaccines.
Additionally, a growing body of basic research has found that the spike protein on the surface of the SARS-CoV-2 virus, which is a component of the vaccine, not only binds to cell surface receptors, but also causes cardiac cell damage, vascular damage, mitochondrial damage, and induces chronic inflammatory states. It is a toxic protein.
Under these circumstances, it is irrational and potentially damaging to use spike protein to stimulate the body.
Moreover, the rocket-like speed of vaccine development and uncertainty of vaccine safety issues has brought stress and tension among people, which can cause excessive release of stress hormones and reduce the human body’s immune resistance to the virus further.
It is good to be proactive, but we should follow the nature of the epidemic, and treat people as fellow humans rather than “living beings.” With a pandemic response, we should first ensure that people eat, drink, and rest well, and are emotionally stable. We shouldn’t over-medicate and over-react.
The Third Lesson Learned: Failure of Transparency
The September 2021 issue of the New England Journal of Medicine published a study of Pfizer’s BNT162b2 mRNA COVID-19 vaccine over six months. There was one case of cardiac arrest in the placebo group, but 4 cases in those who received the vaccine. But this data was not transparently discussed in the main article, but in the supplementary appendix.
Although the numbers are too small to be statistically significant, from a pharmacovigilance perspective, this is an unusual safety signal and due diligence should be further made.
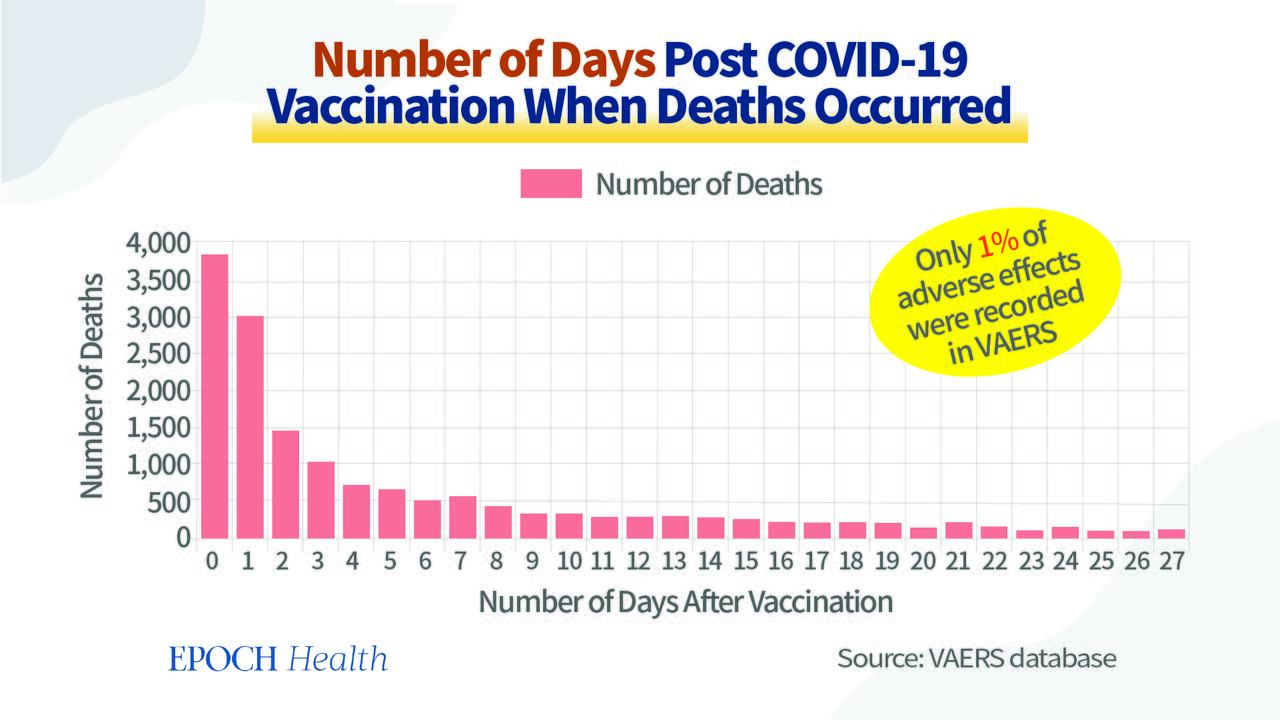
As of Sept. 23, 2022, the VAERS COVID Vaccine Adverse Event Reports database has recorded 1,424,789 cases of adverse events with 31,214 deaths, most of which occurred within one to seven days of vaccination. The unusual short time to death strongly indicates the causal role of vaccines in those death cases.
{kind=link}
A Nordic study published in April 2022 showed that the mRNA vaccine was associated with an increased risk of myocarditis, with the highest risk in young men aged 16 to 24. The number of myocarditis episodes increased 4 to 7 cases per 100,000 young men within 28 days of the second Pfizer vaccination and increased 9 to 28 cases per 100,000 young men within 28 days of the second Modena vaccination.
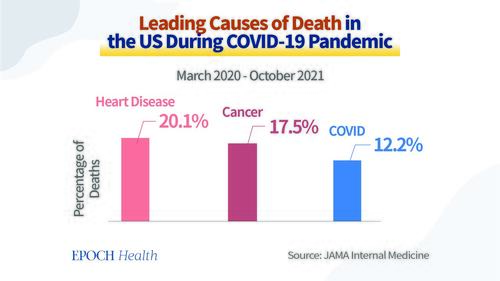
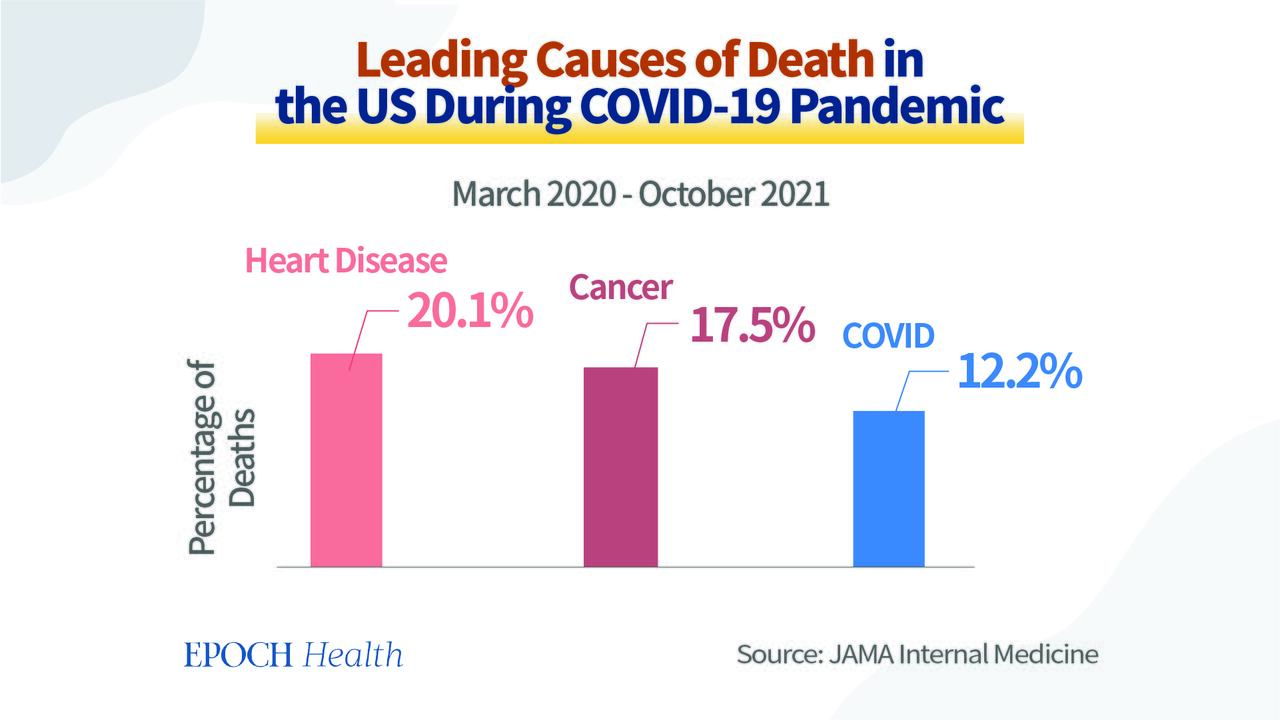
A study published in the July 2022 issue of JAMA Internal Medicine reported that the leading cause of death in the United States during the pandemic period of March 2020 to October 2021 was heart disease.
{kind=link}
A report published in April 2022 in Nature found a 25 percent increase in cardiac arrest and acute coronary syndrome among young people aged 16 to 39. This phenomenon is closely related to the mRNA vaccines but not the COVID-19 infection.
Renowned British cardiologist Dr. Aseem Malhotra, who used to support the mRNA vaccine, published two articles in the Journal of Insulin Resistance calling for a halt on mRNA vaccine. What changed his mind?
As a supporter of the mRNA vaccine, Dr. Malhotra volunteered at vaccine centers and was one of the first people to receive two doses of the Pfizer mRNA vaccine. He also advised his patients and those around him to get the shot.
His father, Dr. Kailand Chand, former Vice President of the British Medical Association (BMA) and a general practitioner, suffered a cardiac arrest at home on July 26, 2021, six months after he received two doses of Pfizer mRNA vaccine.
The autopsy revealed that two of his father’s three major coronary arteries were severely obstructed, with the left anterior descending branch 90 percent obstructed and the right coronary artery 75 percent obstructed.
His father led an active lifestyle and was healthier than most men of his age. Even during the pandemic lockdown, he meditated regularly and walked an average of 10,000 to 15,000 steps a day.
Malhotra suspected that his father’s death was related to the vaccination and subsequently discovered the problem with the vaccine. He called for an end to the vaccination, but it was already too late.
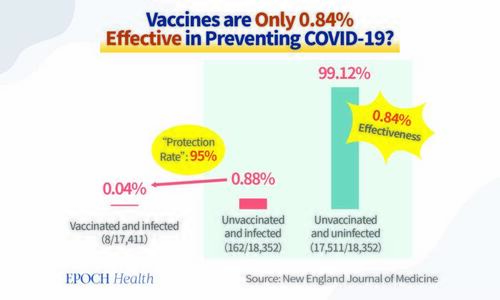
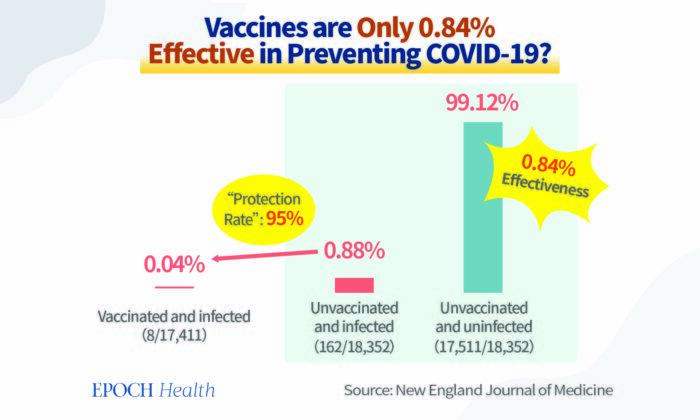
The Truth About ‘95% Effectiveness’: 95 out of 100 Protected?
In terms of the vaccine’s effectiveness, news reports around the world claim that the vaccine is “95 percent effective.” Most doctors explain to the public that “if 100 people are vaccinated, then 95 will be protected from infection.”
But that is not the case at all.
According to the paper published on Dec. 10, 2020 in the New England Journal of Medicine studied the safety and efficacy of Pfizer’s BNT162b2 mRNA Covid-19 vaccine. Of the 18,325 unvaccinated people, there were 162 symptomatic infections. The infection rate was 0.88 percent. Among the 18,198 vaccinated people, there were 8 infections. The infection rate was 0.04 percent. Then it concluded that “the vaccine was 95% effective in preventing Covid-19.”
However, most people overlooked the fact that 99.12 percent of the population was not infected despite being unvaccinated.
For the total population, the vaccine actually protects only 0.84 percent of the population, which is the real absolute protection rate.
So the real “absolute protection” is out of 10000 people vaccinated, only 84 people (0.84%) will be protected, but not the 95 out of 100 people will be protected, which is a relative protection.
Had we known the facts of absolute protection, would we have worried about creating a vaccine so much? We would not have such high hopes that a vaccine would resolve the pandemic. The vaccine mandate would not be so solid at the beginning.
Instead, we would be more rational to seek natural ways to boost immunities so as to prevent the virus in a more feasible and easy way.