- Authors: Ben Hu, Hua Guo, Peng Zhou & Zheng-Li Shi Nature Reviews Microbiology volume 19, pages141–154 (2021)
Abstract
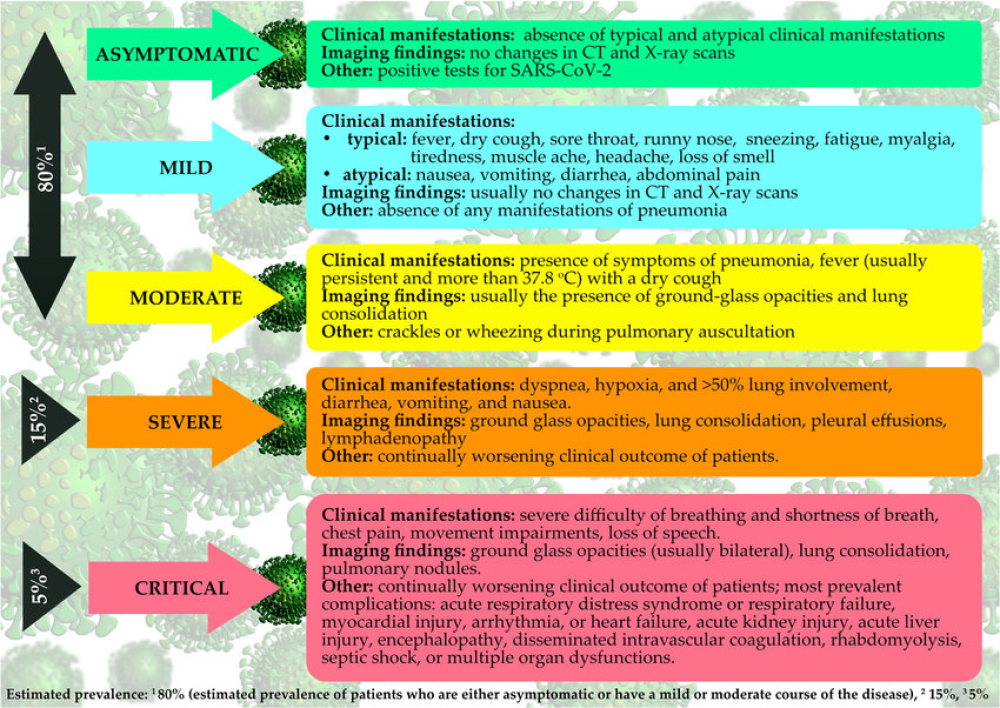
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly transmissible and pathogenic coronavirus that emerged in late 2019 and has caused a pandemic of acute respiratory disease, named ‘coronavirus disease 2019’ (COVID-19), which threatens human health and public safety. In this Review, we describe the basic virology of SARS-CoV-2, including genomic characteristics and receptor use, highlighting its key difference from previously known coronaviruses. We summarize current knowledge of clinical, epidemiological and pathological features of COVID-19, as well as recent progress in animal models and antiviral treatment approaches for SARS-CoV-2 infection. We also discuss the potential wildlife hosts and zoonotic origin of this emerging virus in detail.
Introduction
Coronaviruses are a diverse group of viruses infecting many different animals, and they can cause mild to severe respiratory infections in humans. In 2002 and 2012, respectively, two highly pathogenic coronaviruses with zoonotic origin, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), emerged in humans and caused fatal respiratory illness, making emerging coronaviruses a new public health concern in the twenty-first century1. At the end of 2019, a novel coronavirus designated as SARS-CoV-2 emerged in the city of Wuhan, China, and caused an outbreak of unusual viral pneumonia. Being highly transmissible, this novel coronavirus disease, also known as coronavirus disease 2019 (COVID-19), has spread fast all over the world2,3. It has overwhelmingly surpassed SARS and MERS in terms of both the number of infected people and the spatial range of epidemic areas. The ongoing outbreak of COVID-19 has posed an extraordinary threat to global public health4,5. In this Review, we summarize the current understanding of the nature of SARS-CoV-2 and COVID-19. On the basis of recently published findings, this comprehensive Review covers the basic biology of SARS-CoV-2, including the genetic characteristics, the potential zoonotic origin and its receptor binding. Furthermore, we will discuss the clinical and epidemiological features, diagnosis of and countermeasures against COVID-19.
Emergence and spread
In late December 2019, several health facilities in Wuhan, in Hubei province in China, reported clusters of patients with pneumonia of unknown cause6. Similarly to patients with SARS and MERS, these patients showed symptoms of viral pneumonia, including fever, cough and chest discomfort, and in severe cases dyspnea and bilateral lung infiltration6,7. Among the first 27 documented hospitalized patients, most cases were epidemiologically linked to Huanan Seafood Wholesale Market, a wet market located in downtown Wuhan, which sells not only seafood but also live animals, including poultry and wildlife4,8. According to a retrospective study, the onset of the first known case dates back to 8 December 2019 (ref.9). On 31 December, Wuhan Municipal Health Commission notified the public of a pneumonia outbreak of unidentified cause and informed the World Health Organization (WHO)9 (Fig. 1).
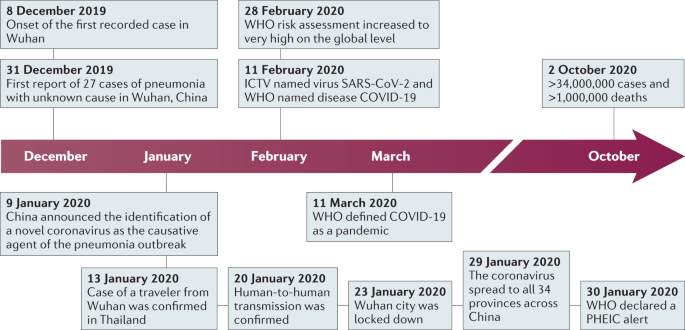
By metagenomic RNA sequencing and virus isolation from bronchoalveolar lavage fluid samples from patients with severe pneumonia, independent teams of Chinese scientists identified that the causative agent of this emerging disease is a betacoronavirus that had never been seen before6,10,11. On 9 January 2020, the result of this etiological identification was publicly announced (Fig. 1). The first genome sequence of the novel coronavirus was published on the Virological website on 10 January, and more nearly complete genome sequences determined by different research institutes were then released via the GISAID database on 12 January7. Later, more patients with no history of exposure to Huanan Seafood Wholesale Market were identified. Several familial clusters of infection were reported, and nosocomial infection also occurred in health-care facilities. All these cases provided clear evidence for human-to-human transmission of the new virus4,12,13,14. As the outbreak coincided with the approach of the lunar New Year, travel between cities before the festival facilitated virus transmission in China. This novel coronavirus pneumonia soon spread to other cities in Hubei province and to other parts of China. Within 1 month, it had spread massively to all 34 provinces of China. The number of confirmed cases suddenly increased, with thousands of new cases diagnosed daily during late January15. On 30 January, the WHO declared the novel coronavirus outbreak a public health emergency of international concern16. On 11 February, the International Committee on Taxonomy of Viruses named the novel coronavirus ‘SARS-CoV-2’, and the WHO named the disease ‘COVID-19’ (ref.17).
The outbreak of COVID-19 in China reached an epidemic peak in February. According to the National Health Commission of China, the total number of cases continued to rise sharply in early February at an average rate of more than 3,000 newly confirmed cases per day. To control COVID-19, China implemented unprecedentedly strict public health measures. The city of Wuhan was shut down on 23 January, and all travel and transportation connecting the city was blocked. In the following couple of weeks, all outdoor activities and gatherings were restricted, and public facilities were closed in most cities as well as in countryside18. Owing to these measures, the daily number of new cases in China started to decrease steadily19.
However, despite the declining trend in China, the international spread of COVID-19 accelerated from late February. Large clusters of infection have been reported from an increasing number of countries18. The high transmission efficiency of SARS-CoV-2 and the abundance of international travel enabled rapid worldwide spread of COVID-19. On 11 March 2020, the WHO officially characterized the global COVID-19 outbreak as a pandemic20. Since March, while COVID-19 in China has become effectively controlled, the case numbers in Europe, the USA and other regions have jumped sharply. According to the COVID-19 dashboard of the Center for System Science and Engineering at Johns Hopkins University, as of 11 August 2020, 216 countries and regions from all six continents had reported more than 20 million cases of COVID-19, and more than 733,000 patients had died21. High mortality occurred especially when health-care resources were overwhelmed. The USA is the country with the largest number of cases so far.
Although genetic evidence suggests that SARS-CoV-2 is a natural virus that likely originated in animals, there is no conclusion yet about when and where the virus first entered humans. As some of the first reported cases in Wuhan had no epidemiological link to the seafood market22, it has been suggested that the market may not be the initial source of human infection with SARS-CoV-2. One study from France detected SARS-CoV-2 by PCR in a stored sample from a patient who had pneumonia at the end of 2019, suggesting SARS-CoV-2 might have spread there much earlier than the generally known starting time of the outbreak in France23. However, this individual early report cannot give a solid answer to the origin of SARS-CoV-2 and contamination, and thus a false positive result cannot be excluded. To address this highly controversial issue, further retrospective investigations involving a larger number of banked samples from patients, animals and environments need to be conducted worldwide with well-validated assays.
For More Information: https://www.nature.com/articles/s41579-020-00459-7