Authors: Moraschini V1, Reis D1, Sacco R2, Calasans-Maia MD3
COVID‐19 is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) that currently presents the greatest, most challenging health concern worldwide. Since the first reports of the disease in December 2019, clinicians and scientists have endeavored to understand the main symptoms, risk factors, and prognosis of the disease (Wynants et al., 2020). Although a significant portion of the infected population remains asymptomatic, many COVID‐19‐infected individuals develop symptoms that vary from mild to severe (Stasi et al., 2020).
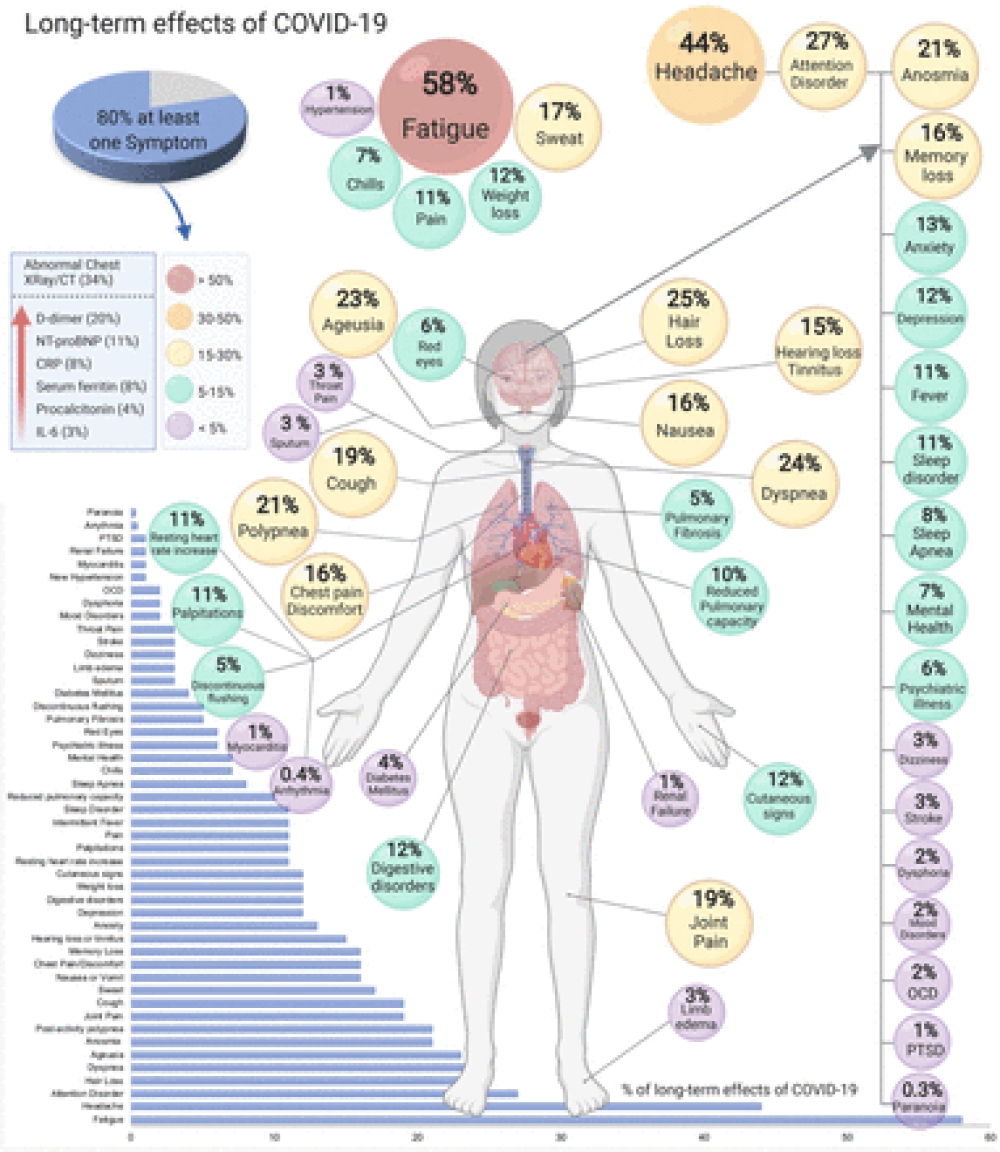
Some patients may experience long‐term effects of COVID‐19, which persist for two or more weeks after the onset of the disease (Tenforde et al., 2020). Loss of taste (ageusia) and smell (anosmia) are symptoms that have drawn substantial attention from researchers because of their high prevalence in the early stages of the disease (Eliezer et al., 2020; Gane et al., 2020). However, recent studies have observed persistent dysgeusia and anosmia following recovery from COVID‐19 infection (Andrews et al., 2020; Garrigues et al., 2020; Panda et al., 2020).
The aim of this study was to estimate the prevalence of dysgeusia and anosmia in studies that assessed the long‐term effects of COVID‐19. Four databases (PubMed/MEDLINE, EMBASE, Scopus, and Lilacs) were searched for articles without any restrictions regarding language, and the inclusion criteria were based on the PECO strategy (Morgan et al., 2018). This review included studies that analyzed the prevalence of persistent symptoms (>30 days) of anosmia and dysgeusia in patients who had COVID‐19. There were no language restrictions. Two independent review authors (V.M. and M.D.C.M.) conducted the search‐and‐screening process, commencing with the analysis of titles and abstracts. Next, full papers were selected for careful reading and matched with the eligibility criteria for subsequent data extraction. The search strategy is described in Table S1.
Regarding the quality of the analyzed studies and risk of bias, one study was classified as low quality (Andrews et al., 2020), two as satisfactory (Garrigues et al., 2020; Horvath et al., 2020), and five as of high quality (Carfì et al., 2020; Carvalho‐Schneider et al., 2020; Chopra et al., 2020; Galván‐Tejada et al., 2020; Panda et al., 2020). The analyses can be viewed in Table S2.
The two review authors (V.M. and M.D.C.M.) independently performed risk‐of‐bias and study quality analyses. The Newcastle–Ottawa Scale (Lo et al., 2014) was used in the analysis of non‐randomized studies. For data analysis, the effects reported in one simple arm were estimated by dividing the number of patients with each symptom by the total number of patients with COVID‐19 in the sample and then by multiplying by 100 to estimate the percentage. The prevalence with 95% confidence intervals (CIs) was presented using the software Comprehensive Meta‐Analysis (BioStat).
A total of eight observational studies were selected for this study. Six cohort studies (Andrews et al., 2020; Carfì et al., 2020; Carvalho‐Schneider et al., 2020; Chopra et al., 2020; Horvath et al., 2020; Panda et al., 2020), one cross‐sectional study (Garrigues et al., 2020), and one case–control study (Galván‐Tejada et al., 2020) were included in this study (Figure S1). The studies analyzed 1,483 patients (773 male and 710 female) with a mean age of 48.3 ± 11.2. All patients were diagnosed with COVID‐19 through reverse transcription polymerase chain reaction (RT‐PCR) and exhibited mild, moderate, or severe symptoms. The mean overall follow‐up time was 60.7 days. The main data for each study are shown in Table Table11.
For More Information: https://europepmc.org/article/PMC/PMC8242542