Authors: Zhen W Mei, Xander M R van Wijk, Huy P Pham, Maximo J Marin
The Journal of Applied Laboratory Medicine, Volume 6, Issue 5, September 2021, Pages 1305–1315, https://doi.org/10.1093/jalm/jfab042Published: 13 June 2021
Abstract
Background
COVID-19, the disease caused by SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) can present with symptoms ranging from none to severe. Thrombotic events occur in a significant number of patients with COVID-19, especially in critically ill patients. This apparent novel form of coagulopathy is termed COVID-19-associated coagulopathy (CAC), and endothelial derived von Willebrand factor (vWF) may play an important role in its pathogenesis.Content
vWF is a multimeric glycoprotein molecule that is involved in inflammation, primary and secondary hemostasis. Studies have shown that patients with COVID-19 have significantly elevated levels of vWF antigen and activity, likely contributing to an increased risk of thrombosis seen in CAC. The high levels of both vWF antigen and activity have been clinically correlated with worse outcomes. Furthermore, the severity of a COVID-19 infection appears to reduce molecules that regulate vWF level and activity such as ADAMTS-13 and high-density lipoproteins (HDL). Finally, studies have suggested that patients with group O blood (a blood group with lower baseline levels of vWF) have a lower risk of infection and disease severity compared to other ABO blood groups; however, more studies are needed to elucidate the role of vWF.Summary
CAC is a significant contributor to morbidity and mortality. Endothelial dysfunction with the release of prothrombotic factors, such as vWF, needs further examination as a possible important component in the pathogenesis of CAC.von Willebrand Factor, COVID-19, coagulopathy, endothelial injury, thrombosisIssue Section: Mini-review
Introduction and Background
COVID-19 Pandemic
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was initially identified in Wuhan, China in 2019. COVID-19, the disease caused by SARS-CoV-2, quickly evolved into a global pandemic. According to the Johns Hopkins COVID-19 Dashboard, there were more than 20 million confirmed cases and almost 350,000 deaths in the US alone, by the end of 2020. Although COVID-19 may present with a variety of symptoms, a large majority of infected individuals may have none to only mild symptoms (1). However, the mortality rate is dominated by a subset of patients with severe respiratory failure that meet the criteria for acute respiratory distress syndrome (ARDS) and require respiratory support (1, 2). The development of severe disease is related to interstitial viral pneumonia, systemic inflammation, respiratory failure, and multiorgan dysfunction (3).Impact Statement
COVID-19 is a global pandemic with no current effective treatment. COVID-19-associated coagulopathy contributes to patient morbidity and mortality. von Willebrand factor (vWF) may play an important role in the pathogenesis of this coagulopathy. Currently, available studies have demonstrated that patients with COVID-19 have significantly elevated levels of vWF antigen and activity as well as reduced regulatory molecules, which could contribute to an increased risk of thrombosis seen in patients who develop coagulopathy. Elucidation of vWF role in patients with COVID-19 may offer additional insights into developing novel therapies for this disease.
Viral Pathophysiology
SARS-CoV-2 preferentially binds to host cells that express the angiotensin-converting enzyme-2 receptor (ACE2) through the viral spike protein structure. The initiation and progression of the SARS-CoV-2 infection is likely dependent on a combination of factors, including, but not limited to, host cell expression of ACE2, anatomic contiguity with the environment, inoculation dose at the time of exposure, and the host immune response to the infection. In general, the initial infection by the SARS-CoV-2 virus targets the cells of the respiratory system such as nasal or bronchial epithelial cells and pneumocytes. However, if the severity of the infection progresses to a systemic inflammatory phase, the mechanism is likely a complex combination of the virus entering the blood stream, infection of other cells expressing ACE2 receptors, tissue/organ specificity, and the inflammatory milieu. However, the extent to which each factor contributes to the systemic severity remains unclear. Additionally, in severe COVID-19 cases, endothelial cells (ECs), which also express ACE2 receptors, are activated, leading to endothelial dysfunction and possible injury that parallels clinical manifestations, such as coagulopathy and prothrombotic tendency (4).
COVID-19 Associated Coagulopathy
It is clear that a significant component of the observed morbidity and mortality is directly related to lung injury as supported by COVID-19 related autopsies (5, 6). The predominant pattern of injury was found to be diffuse alveolar damage, which includes hyaline membrane formation, capillary congestion, inflammation, and pneumocyte necrosis. In addition, the study also identified platelet-fibrin thrombi in small arterial vessels in 87% of their cases (6). A more recent, albeit small, series showed that all COVID-19 related autopsies demonstrated platelet-fibrin thrombi in multiple organs, including the liver, kidney, heart, and lungs (5). Another autopsy case series compared lung tissue from equally severe, age-matched patients with ARDS with either COVID-19 or influenza A (H1N1) and found that alveolar capillary microthrombi were more prevalent in COVID-19 than influenza (7). This study also observed that COVID-19 lung tissue showed significant EC injury associated with intracellular SARS-CoV-2 infection (7). Furthermore, there is some evidence to suggest that COVID-19 associated coagulopathy (CAC) might be different from other coagulopathic conditions, such as disseminated intravascular coagulation (DIC) and thrombotic microangiopathy (TMA), which are associated with other underlying causes such as infections, malignancy, autoimmune, and hereditary diseases (Table 1) (8). Taken together, the data indicate that a distinct coagulopathy may be occurring in COVID-19 patients, particularly those with severe symptoms.
Laboratory data in COVID-19 and other coagulopathies.
| Platelet count | D-dimer | PT/INR; aPTT | Fibrinogen | Antithrombin activity | Complement activation | Inflammatory cytokines | ADAMTS-13 | vWF antigen | |
|---|---|---|---|---|---|---|---|---|---|
| Normal | within reference range | within reference range | within reference range | within reference range | within reference range | within reference range | within reference range | within reference range | within reference range |
| COVID-19 | generally, mildly elevated early and decreases as severity increases | elevated | no change to mildly elevated | elevated | no change | increased activation, may result in lower antigen levels due to consumption | elevated | mildly decreased | elevated |
| DIC/SIC | decreased | elevated | elevated | no change to decreased | decreased | no increase | elevated | normal | decreased |
| TTP | Severely decreased | no change to elevated | no change to elevated | no change | no change | normal to mildly increased | decreased | severely decreased | normal to mildly elevated |
| HUS | decreased | no change to elevated | no change to elevated | no change | no change | usually mildly increased but may be normal | decreased | normal | normal to mildly elevated |
| Atypical HUS | decreased | no change to elevated | no change to elevated | no change | no change | moderate to severely increased | decreased | normal to moderately decreased | normal to mildly elevated |
Normal values will vary among laboratories due to varying methodologies and reagents. Given that there are multiple markers for complement activation, inflammation, and acute phase reactants, reference ranges for these (patho)-physiological events are not provided. Of note, ADAMTS13 measurement is generally the reliable biomarker distinguishing TTP from HUS/atypical HUS. HUS can be distinguished from aHUS if the patient has history of Shiga-toxin or Streptococcus exposure. Other biomarkers may be overlapping in the spectrum from DIC/SIC to TTP/HUS/aHUS. DIC: disseminated intravascular coagulation, SIC: sepsis-induced coagulopathy, TMA: thrombotic microangiopathy, TTP: thrombotic thrombocytopenia purpura, aHUS: atypical hemolytic uremic syndrome, PT: prothrombin time, aPTT: activated partial thromboplastin time, vWF: von Willebrand factor. Adapted from Iba et al. (8).Open in new tab
Incidence of CAC, especially in severe COVID-19 cases, was apparent from early reports in Wuhan (9). A number of studies have shown that the development of CAC is an important prognostic indicator of poor outcomes (10–12). One study evaluated the rate of arterial and venous thrombotic events in COVID-19 pneumonia patients admitted into the intensive care unit (ICU) and found that the incidence of thrombotic events in 184 patients was 49% (after adjustment for competing risk of death) despite receiving routine pharmacologic thromboprophylaxis; not surprisingly, these thrombotic complications led to a higher risk of death (13). Additional studies have shown similar incidence rates of thrombotic events in COVID-19 ICU patients (14, 15). Collectively, clinical studies suggest that CAC leads to a prothrombotic state even with standard pharmacologic thromboprophylaxis treatment.
Laboratory Patterns
In general, CAC is characterized by mild thrombocytopenia, slight prolongation of the prothrombin time (PT), high levels of D-dimer, and elevated fibrinogen (8, 12, 16) (Table 1). Recent International Society for Thrombosis and Hemostasis (ISTH) interim guidance recommends monitoring these 4 parameters in the management of patients with CAC. D-dimer was designated the highest level of priority as many studies have shown that elevated levels are associated with increasing severity of disease and mortality risk (3, 10, 11, 17–20). These studies reported a range of associations of higher D-dimer levels in COVID patients, including greater risk of mortality (3, 11, 18), increased disease severity (10, 11), increased incidence of pulmonary emboli (17), and need for intensive care (20). Based on this data, clinical services can order a baseline D-dimer level to determine the current morbidity and mortality risk that a COVID-19 patient carries and can follow a D-dimer level to predict progression to more severe disease.
D-dimer is a breakdown product of mature clots (cross-linked fibrin mesh) that undergoes fibrinolysis. Though some studies reported data where the association with D-dimer and death may not be as compelling (21, 22), D-dimer levels do play a role during the follow-up and treatment of patients with CAC. There is, however, another biomarker, von Willebrand factor (vWF), which may also play an important role in the evaluation of CAC patients due to its direct relationship to hemostasis, inflammation, and EC activation/injury, which are all important aspects of COVID-19 pathogenesis. The biological role of vWF and its association with CAC will be the focus of the remainder of this review.
vWF Physiology and Laboratory Testing
vWF Biology
vWF is a multimeric glycoprotein ranging from 2 to >60 prepropolypeptide units that are each 2138 amino acids in length. The vWF propeptide sequence serves to align 2 units together to allow proper cross-linking during the multimerization process. Further post-translational modification leads to removal of the propeptide sequence as well as glycosylation, including the addition of blood group determinants. This addition of an A or B blood group determinant only occurs during EC glycosylation. Following these processes, a heterogenous mix of ultra-large-vWF (UL-vWF) molecules are synthesized and stored in megakaryocytes and ECs, respectively, in alpha granules and Weibel–Palade bodies (WPB). Additionally, other processing components such as vWF propeptides are found in the WPB of ECs. Although platelets do play an important role in both storage and secretion of vWF, this review will focus on ECs.
When ECs are activated, UL-vWF molecules are released and can either remain free-floating in the plasma or localized on endothelial surfaces. UL-vWF have greater prothrombotic activity than smaller vWF multimers. Therefore, as UL-vWF molecules are secreted, ADAMTS-13 (a disintegrase and metalloproteinase with a thrombospondin type 1 motif, member 13), cleaves vWF into smaller multimers to mitigate unwanted thrombus formation and leads to a variation in the sizes of vWF found both in the plasma and on endothelial surfaces. Elevated vWF activity levels depend on the presence of the largest vWF multimers and activation by shear stress in the circulatory system. vWF responds to shear stress by unfolding and exposing sites for activity such as self-association, platelet binding, and ADAMTS-13 cleavage. Accordingly, the imbalance of these components may lead to a prothrombotic state.
Role in Primary Hemostasis
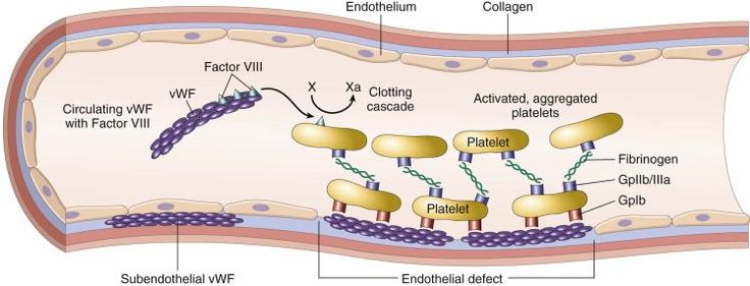
Primary hemostasis is the process of the platelet clot formation at the site of blood vessel injury. For proper primary hemostasis to occur, platelet adhesion and aggregation must occur. During platelet adhesion at the site of blood vessel injury, platelets can bind directly to the exposed subendothelial collagen (via GPIa-IIa or GPVI receptors) or indirectly via vWF. In the latter case, platelets bind to the vWF molecule via the platelet glycoprotein Ib-V-IX receptor (GPIb) while vWF is bound to subendothelial collagen. Additionally, vWF also promotes platelet aggregation (platelet–platelet interaction) by binding to platelet surface receptor GPIIb/IIIa. Although GPIIb/IIIa is better known as a fibrinogen receptor, it can bind to both fibrinogen and vWF. In summary, vWF plays a vital role in platelet adhesion and aggregation in clot formation.
Role in Secondary Hemostasis
vWF also performs an important role in secondary hemostasis. Secondary hemostasis involves coagulation factors and the coagulation cascade to produce a fibrin meshwork at the site of vessel injury. vWF facilitates the secondary hemostasis process in two ways. First, vWF serves as a carrier protein for Factor VIII, extending Factor VIII’s half-life in the plasma. Although this may initially seem trivial, the vWF carrier activity stabilizes Factor VIII and significantly extends its half-life 4 to 6-fold. Second, it releases and concentrates Factor VIII at the site of injury. Factor VIII is a clotting factor that, when activated, complexes with other factors to ultimately produce fibrin. To highlight the significance of vWF in this process, mutations affecting the vWF binding site for Factor VIII leads to decreased levels of Factor VIII, known as Type 2N von Willebrand disease (vWD), resulting in a clinical presentation similar to hemophilia A, which is a bleeding disorder that occurs when an individual lacks the ability to produce adequate amounts of Factor VIII for proper clotting.
vWF, Inflammation, and Endothelial Activation/Injury
During the inflammatory process, various chemical mediators are released. These inflammatory molecules activate ECs to release their WPB contents, including vWF and other molecules such as P-selectin, which has been directly linked to leukocyte recruitment (23, 24). In addition, UL-vWF molecules that remain bound to EC surface will subsequently bind platelets and may have the ability to act as a molecular surface for leukocyte interaction (25). With increased release of vWF, the inflammatory process is expected to induce a prothrombotic state. Studies show that inflammation enhances vWF self-association, which may lead to increased adhesiveness of platelets while decreasing ADAMTS-13 cleavage (24). Additionally, high-density lipoprotein (HDL) decreases during inflammation in both chronic and acute phases. HDL may play a vital role in preventing shear stress-induced vWF self-association, thus decreasing prothrombotic risk under normal circumstances (24). This concept will become a point of discussion later in the review. In summary, the data indicate that during the inflammatory process there is an increased thrombotic risk due to the imbalance of increased vWF and activity levels via EC activation and reduced ADAMTS-13 activity.
Laboratory Testing of vWF
To understand the studies that will be mentioned in connection with CAC, it is important to briefly discuss basic vWF laboratory testing. There are 3 basic tests performed to assess vWF; the exact methods may vary between manufacturers for those that are highly automated but the fundamental parameters rest on testing vWF quantity, activity, and multimer size.
The quantity of the vWF level in a specimen is commonly referred to as antigenic testing (vWF:Ag). An immunoturbidimetric method is commonly used for vWF:Ag measurement. However, the details of the assays vary by manufacturer. This allows for quantitative determination of the physical presence of the molecule without assessment of function. ABO blood typing and Factor VIII levels are also performed concurrently; it is well documented that individuals of blood group O have physiologically lower levels of vWF, and therefore Factor VIII (since vWF binds and stabilizes it) levels are also slightly lower than individuals of non-O blood groups (see the “vWF Association with Blood Type” section).
The quality of present vWF is known as functional or activity testing; this involves testing the ability of vWF to bind to platelet receptor GPIb, collagen, and Factor VIII (vWF:RCo). There are a number of assays and methods that revolve around testing the ability of vWF to bind its natural physiologic substrates (with or without ristocetin). Depending on the substrate used to assess its binding function, these tests will often carry an acronym such as vWF:Ac, vWF:RCo, vWF:Co, or vWF:VIII. It is important to note that there are important and distinct differences amongst these tests; however, this is beyond the scope of the review.
Additionally, the qualitative variation of vWF multimers is performed to visualize the presence and size distribution of vWF located in the plasma using gel electrophoresis and vWF labeling. This assessment is important since multimer presence and size is directly correlated to the function and activity level of the vWF molecule.
Finally, although not a laboratory test, the results of the activity and antigenic assays may be juxtaposed to obtain the ratio of vWF activity to antigen (RCo:Ag ratio). A ratio that is less than 0.5–0.7 would indicate that a qualitative defect in the vWF molecules is likely and this helps categorize the pattern and subtypes of vWD, if present.
Examination of vWF in COVID-19 Associated Coagulopathy
Endothelial Activation and vWF
As a molecule present in ECs that plays a fundamental role in hemostasis and thrombosis, vWF is a reasonable candidate marker to consider when monitoring clinical issues related to endothelial injury and coagulopathy in COVID-19. Early studies duly noted that D-dimer levels were an important prognostic marker in COVID-19. However, studies also began to recognize and demonstrate that significantly elevated levels of vWF were also present (14, 16, 19, 26). Further, studies then recognized that vWF activity is also increased and that ADAMTS-13 activity levels are relatively mild to moderately reduced, leading to an imbalance favoring thrombosis (27, 28). Similarly, in a well-recognized pathological entity, thrombotic thrombocytopenic purpura (TTP) is associated with reduced activity levels of ADAMTS-13. TTP is generally due to an extremely hindered or absent ADAMTS-13 activity by either an acquired inhibitor or congenital absence. The decreased activity levels of ADAMTS-13 result in an excess of overactive UL-vWF multimers that promote microthrombi formation.
However, in contrast to TTP, the mild to moderately decreased ADAMTS-13 activity levels observed in CAC may not lead to excessive UL-vWF. Thus, it is important to distinguish that activity levels of ADAMTS-13 may not be low enough in CAC cases to detect an excessive increase in UL-vWF as seen in severe deficiency such as in TTP. In line with this, a recent study showed decreased activity levels of ADAMTS-13 in patients with severe COVID-19 but found no evidence of UL-vWF multimers in the plasma (29). Further, the authors of this study emphasized the significance of the elevated vWF:Ag to ADAMTS-13 activity ratio in association with increasing severity of disease. This suggests that an increased risk of thrombosis seen in patients with COVID-19 may, in part, be due to a relative decrease of ADAMTS-13 activity rather than an absolute decrease as seen in TTP.
The high levels of both vWF antigen and activity have been correlated clinically with increased thrombotic events (14), increased likelihood for treatment in ICUs (19), and increased need for oxygen support (26), as well as correlated with other laboratory testing such as decreased clotting times, increased clot formation velocities as demonstrated by whole blood viscoelastic testing (16) and increased levels of other markers of platelet and endothelial activation, such as Factor VIII and thrombomodulin (16, 19, 26–28, 30). As new biomarkers to assess CAC severity emerge, reexamining the synthetic pathway of vWF may have some utility. One promising avenue is to examine levels of vWF propeptide; its physiologic role in the multimerization process would suggest that elevated levels of vWF propeptide indicate elevated vWF release. In addition, a greater level of increase in vWF and propeptide in comparison to an increase in Factor VIII suggest that this is due to release of vWF from pulmonary ECs involved in the COVID-19 pathophysiologic process (31). The ratio of propeptide levels to vWF levels can also examined; this ratio seems to decrease with disease progression suggesting that while the propeptide is cleared normally, levels of vWF may stay elevated due to decreased clearance (29). Further examination of propeptide levels in patients with COVID-19 are indicated to elucidate these possible relationships.
High-Density Lipoprotein and vWF
Aside from endothelial activation and injury, a more indirect mechanism may contribute to increased vWF activity levels. In general, infection leads to an inflammatory state and, as mentioned previously, this decreases HDL levels. Although most commonly known for its important role in preventing atherosclerotic disease, additional physiologic functions include activity as an antiinflammatory, antiapoptotic, and antioxidant agent. However, lesser-known roles include preventing thrombosis through binding to ECs to ramp up nitric oxide (a vasodilatory molecule) production and preventing shear stress-induced vWF self-association, thus decreasing prothrombotic risk (24, 32). Interestingly, a retrospective analysis of total cholesterol, LDL and HDL levels of patients in Changsha, China showed that HDL levels were lower in patients with COVID-19 than normal and patients with severe disease had lower HDL levels than patients with mild disease (33). Beyond the general infectious inflammatory state that may reduce HDL levels, a study showed that patients with COVID-19 had reduced apolipoprotein A1 (ApoA1) levels, which is a major protein component of HDL molecules (34). The study also showed that as patients went from nonsevere to severe disease, apolipoprotein decreased. Indeed, it has been shown, both in vivo and vitro models, that ApoA1 prevents vWF self-association and binding to vessel walls (32). Additional studies in the future could shed light on the role of HDL in CAC patients and possibly lead to novel treatment options.
vWF Association with Blood Type and COVID-19 Susceptibility
If increased levels of vWF can be monitored as a marker of endothelial damage and used to predict prognosis in patients with COVID-19, then decreased levels of vWF may be protective. One naturally existing population of patients who have baseline lower levels of vWF are patients of blood group O. Group O individuals naturally have a baseline level of vWF ∼25% less than the non-group O cohort (blood groups A and B). Although the exact molecular mechanism by which group O individuals have lower vWF levels is not fully elucidated, it has been hypothesized that perhaps theadditional glycosylation status, which occurs within ECs, by non-group O individuals prevents the activity of ADAMTS-13 to cleave vWF. This leads to reduced clearance and an increased half-life that is demonstrated by baseline higher levels of vWF when compared to group O individuals (31).
Initial data from China found a greater than expected proportion of group A and a smaller than expected proportion of group O individuals among patients with COVID-19. However, this involved a small cohort of patients with limited analysis due to lack of available clinical information (35). Following this, a genome-wide association study on patients in Italy and Spain also found group O individuals to have a lower relative risk than non-group O individuals (36). Another study showed a similar pattern of this phenomenon in a cohort of patients treated at the New York Presbyterian Hospital System (37). However, conflicting information is reported among these and other studies with some reporting no significant difference in severity and some reporting contradicting patterns in terms of need for mechanical ventilation. Preliminary data from these studies do potentially suggest that the lower vWF levels may be associated with decreased severity of disease in group O patients but more data is needed to clarify this relationship.
Conclusion
CAC is a significant contributor to patient morbidity and mortality. We highlight the role of vWF in CAC and compare and contrast it to the normal physiological response, mild and severe COVID-19 disease, and TTP (Fig. 1). Direct infection of ECs with SARS-CoV-2 and/or activation of ECs due to high levels of inflammatory mediators results in release of prothrombotic factors such as vWF. vWF, bound to the ECs or in plasma, promotes platelet aggregation and thrombus formation. It is likely that multiple mechanisms contribute to an imbalance of the vWF-ADAMTS-13 axis, pushing patients with CAC toward a more prothrombotic tendency. For example, in this review we discussed HDL and role it plays in reducing vWF activity, in which little discussion has been seen in other review articles of CAC and vWF. Nevertheless, the range of clinical presentation may be a reflection of the severity of this imbalance since reports show that though vWF is elevated in patients who are both critically ill and noncritically ill (19), there is a significant difference in vWF and ADAMTS-13 levels in patients who suffer thrombotic events versus those that do not (38). Multiple biomarkers, including vWF-associated proteins such as vWF propeptide and P-selectin, may help demonstrate the level of imbalance, as well as the mechanisms causing the imbalance. This would clarify the roles of therapies that would counter the actions of these prothrombotic molecules, whether by mitigating their release by reducing inflammation, such as N-acetylcysteine (39), or by inhibiting their activity once released or activated, such as caplacizumab (anti-vWF) or crizanlizumab (anti-P-selectin). Regardless, vWF has clearly demonstrated that it plays a role in the progression of CAC in patients with COVID-19, however, to what extent remains unclear. Further studies are needed to elucidate the many roles of vWF and the mechanism by which it becomes imbalanced.Fig. 1 Open in new tabDownload slide
Open in new tabDownload slide
{kind=link}
Proposed mechanism and distinguishing characteristics in mild and severe cases of COVID-19 associated coagulopathy and a comparison to a normal physiological response and thrombotic thrombocytopenic purpura. (A), Normal physiological response to stress and or injury. After endothelial activation, vWF multimers are bound to the endothelial surface, ADAMTS-13 actively cleaves large multimers and HDL assists in the regulation of vWF self-association resulting in well-controlled thrombus formation during a physiologic response. (B), COVID-19 associated coagulopathy in mild disease. Localized infection and minimal systemic inflammation lead to a higher level of endothelial cell activation. Regardless, in this scenario, infection and inflammation remains fairly well regulated. Furthermore, the HDL and ADAMTS-13 mechanisms are mostly intact, leading to only a slight increase of pathologic thrombotic events. (C), COVID-19 associated coagulopathy in severe disease. Infection and or inflammation becomes overwhelmingly dysregulated, leading to an extremely elevated level of endothelial activation. Additionally, both HDL and ADAMTS-13 levels are decreased, leading to a much higher increase risk of pathologic thrombotic events. (D), Thrombotic thrombocytopenia purpura (TTP). In TTP, ADAMTS-13 activity levels are significantly lower than observed in COVID-19 coagulopathy. TTP leads to increased levels of ultralarge and large multimers of vWF. Subsequently, there are increased levels of platelet binding, which leads to highly increased thrombotic risk.
Author Contributions
All authors confirmed they have contributed to the intellectual content of this paper and have met the following 4 requirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; (c) final approval of the published article; and (d) agreement to be accountable for all aspects of the article thus ensuring that questions related to the accuracy or integrity of any part of the article are appropriately investigated and resolved.
Authors’ Disclosures or Potential Conflicts of Interest: Upon manuscript submission, all authors completed the author disclosure form. Disclosures and/or potential conflicts of interest: Employment or Leadership: H.P. Pham, University of Southern California. Consultant or Advisory Role: H.P. Pham, Sanofi Genzyme. Stock Ownership: None declared. Honoraria: H.P. Pham, Alexion. Research Funding: None declared. Expert Testimony: None declared. Patents: None declared.
REFERENCES
1Wu Z , McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020;323:1239.
Google ScholarCrossrefPubMed2Bhatraju PK , Ghassemieh BJ , Nichols M , Kim R , Jerome KR , Nalla AK , et al. COVID-19 in critically ill patients in the Seattle region – case series. N Engl J Med 2020;382:2012–22.
Google ScholarCrossrefPubMed3Zhou F , Yu T , Du R , Fan G , Liu Y , Liu Z , et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020;395:1054–62.
Google ScholarCrossrefPubMed4Libby P , Luscher T. COVID-19 is, in the end, an endothelial disease. Eur Heart J 2020;41:3038–44.
Google ScholarCrossrefPubMed5Amy V , Rapkiewicz XM , Carsons SE , Pittaluga S , Kleiner DE , Berger JS , Thomas S , et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: a case series. EClinicalMedicine 2020;24:100434.
Google ScholarPubMed6Carsana L , Sonzogni A , Nasr A , Rossi RS , Pellegrinelli A , Zerbi P , et al. Pulmonary post-mortem findings in a series of COVID-19 cases from Northern Italy: a two-centre descriptive study. Lancet Infect Dis 2020; 21: 1135–1140.
Google Scholar7Ackermann M , Verleden SE , Kuehnel M , Haverich A , Welte T , Laenger F , et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N Engl J Med 2020;383:120–8.
Google ScholarCrossrefPubMed8Iba T , Levy JH , Connors JM , Warkentin TE , Thachil J , Levi M. The unique characteristics of COVID-19 coagulopathy. Crit Care 2020;24:360.
Google ScholarCrossrefPubMed9Wu C , Chen X , Cai Y , Xia J , Zhou X , Xu S , et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med 2020;180:934.
Google ScholarCrossrefPubMed10Liao D , Zhou F , Luo L , Xu M , Wang H , Xia J , et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: a retrospective cohort study. Lancet Haematol 2020;7:e671–79.
Google ScholarCrossrefPubMed11Yao Y , Cao J , Wang Q , Shi Q , Liu K , Luo Z , et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study. J Intensive Care 2020;8:49.
Google ScholarCrossrefPubMed12Tang N , Li D , Wang X , Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost 2020;18:844–7.
Google ScholarCrossrefPubMed13Klok FA , Kruip M , van der Meer NJM , Arbous MS , Gommers D , Kant KM , et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: an updated analysis. Thromb Res 2020;191:148–50.
Google ScholarCrossrefPubMed14Helms J , Tacquard C , Severac F , Leonard-Lorant I , Ohana M , Delabranche X , et al. ; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med 2020;46:1089–98.
Google ScholarCrossrefPubMed15Lodigiani C , Iapichino G , Carenzo L , Cecconi M , Ferrazzi P , Sebastian T , et al. ; Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 2020;191:9–14.
Google ScholarCrossrefPubMed16Panigada M , Bottino N , Tagliabue P , Grasselli G , Novembrino C , Chantarangkul V , et al. Hypercoagulability of COVID-19 patients in intensive care unit: a report of thromboelastography findings and other parameters of hemostasis. J Thromb Haemost 2020;18:1738–42.
Google ScholarCrossrefPubMed17Leonard-Lorant I , Delabranche X , Severac F , Helms J , Pauzet C , Collange O , et al. Acute pulmonary embolism in patients with COVID-19 at CT angiography and relationship to D-dimer levels. Radiology 2020;296:E189–E91.
Google ScholarCrossrefPubMed18Zhang L , Yan X , Fan Q , Liu H , Liu X , Liu Z , Zhang Z. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J Thromb Haemost 2020;18:1324–9.
Google ScholarCrossrefPubMed19Goshua G , Pine AB , Meizlish ML , Chang CH , Zhang H , Bahel P , et al. Endotheliopathy in COVID-19-associated coagulopathy: evidence from a single-centre, cross-sectional study. Lancet Haematol 2020;7:e575–e82.
Google ScholarCrossrefPubMed20Huang C , Wang Y , Li X , Ren L , Zhao J , Hu Y , et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395:497–506.
Google ScholarCrossrefPubMed21Martin-Rojas RM , Perez-Rus G , Delgado-Pinos VE , Domingo-Gonzalez A , Regalado-Artamendi I , Alba-Urdiales N , et al. COVID-19 coagulopathy: an in-depth analysis of the coagulation system. Eur J Haematol 2020;105:741–750.
Google ScholarCrossrefPubMed22Cummings MJ , Baldwin MR , Abrams D , Jacobson SD , Meyer BJ , Balough EM , et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet 2020;395:1763–70.
Google ScholarCrossrefPubMed23Kawecki C , Lenting PJ , Denis CV. von Willebrand factor and inflammation. J Thromb Haemost 2017;15:1285–94.
Google ScholarCrossrefPubMed24Chen J , Chung DW. Inflammation, von Willebrand factor, and ADAMTS13. Blood 2018;132:141–7.
Google ScholarCrossrefPubMed25Bernardo A , Ball C , Nolasco L , Choi H , Moake JL , Dong JF. Platelets adhered to endothelial cell-bound ultra-large von Willebrand factor strings support leukocyte tethering and rolling under high shear stress. J Thromb Haemost 2005;3:562–70.
Google ScholarCrossrefPubMed26Rauch A , Labreuche J , Lassalle F , Goutay J , Caplan M , Charbonnier L , et al. Coagulation biomarkers are independent predictors of increased oxygen requirements in COVID-19. J Thromb Haemost 2020;18:2942–2953.
Google ScholarCrossrefPubMed27Escher R , Breakey N , Lammle B. ADAMTS13 activity, von Willebrand factor, factor VIII and D-dimers in COVID-19 inpatients. Thromb Res 2020;192:174–5.
Google ScholarCrossrefPubMed28Escher R , Breakey N , Lammle B. Severe COVID-19 infection associated with endothelial activation. Thromb Res 2020;190:62.
Google ScholarCrossrefPubMed29Mancini I , Baronciani L , Artoni A , Colpani P , Biganzoli M , Cozzi G , et al. The ADAMTS13-von Willebrand factor axis in COVID-19 patients. J Thromb Haemost 2021:19;513-521
Google Scholar30Ladikou EE , Sivaloganathan H , Milne KM , Arter WE , Ramasamy R , Saad R , et al. von Willebrand factor (vWF): marker of endothelial damage and thrombotic risk in COVID-19? Clin Med (Lond) 2020;20:e178–e82.
Google ScholarCrossrefPubMed31Ward SE , O’Sullivan JM , O’Donnell JS. The relationship between abo blood group, von Willebrand factor and primary hemostasis. Blood 2020;136:2864–74.
Google ScholarCrossrefPubMed32Chung DW , Chen J , Ling M , Fu X , Blevins T , Parsons S , et al. High-density lipoprotein modulates thrombosis by preventing von Willebrand factor self-association and subsequent platelet adhesion. Blood 2016;127:637–45.
Google ScholarCrossrefPubMed33Wang G , Zhang Q , Zhao X , Dong H , Wu C , Wu F , et al. Low high-density lipoprotein level is correlated with the severity of COVID-19 patients: an observational study. Lipids Health Dis 2020;19:204.
Google ScholarCrossrefPubMed34Shen B , Yi X , Sun Y , Bi X , Du J , Zhang C , et al. Proteomic and metabolomic characterization of COVID-19 patient sera. Cell 2020;182:59–72.e15.
Google ScholarCrossrefPubMed35Zhao J , Yang Y , Huang H , Li D , Gu D , Lu X , et al. Relationship between the ABO blood group and the COVID-19 susceptibility. Clin Infect Dis 2020:ciaa1150.
Google Scholar36Ellinghaus D , Degenhardt F , Bujanda L , Buti M , Albillos A , Invernizzi P , et al. Genomewide association study of severe COVID-19 with respiratory failure. N Engl J Med 2020;383:1522–34.
Google ScholarPubMed37Zietz M , Zucker J , Tatonetti NP. Associations between blood type and COVID-19 infection, intubation, and death. Nat Commun 2020;11:5761.
Google ScholarCrossrefPubMed38Delrue M , Siguret V , Neuwirth M , Joly B , Beranger N , Sene D , et al. Von Willebrand factor/ADAMTS13 axis and venous thromboembolism in moderate-to-severe COVID-19 patients. Br J Haematol 2021;192:1097–100.
Google ScholarCrossrefPubMed39Shi Z , Puyo CA. N-acetylcysteine to combat COVID-19: an evidence review. Ther Clin Risk Manag 2020;16:1047–55.
Google ScholarCrossrefPubMed © American Association for Clinical Chemistry 2021. All rights reserved. For permissions, please email: journals.permissions@oup.com.